
Abstract
Background: In Singapore, the National Electronic Health Record (NEHR) was launched in 2011. The central ethos of the initiative was that of “One Patient, One Health Record”, as NEHR allows registered doctors to review and upload patient data. However, uptake of the system has been slow in the private sector, with only 27% of doctors with private licenses, including general practitioners (GP) and specialists in the ambulatory care setting, accessing it. A questionnaire-based study was therefore conducted to find out the proportion of GP who used NEHR, and the barriers faced by those who do not.
Methods: This study involved a self-administered questionnaire, randomly sampling private GP in Singapore. The questionnaire ascertained the number of GP who used NEHR and gathered their demographic information. A 5-point Likert scale was used to measure the perceived barriers to NEHR use.
Results: Of the 315 responses, multinomial logistics regression showed that solo-practising GP who were >40 years old and who had practised for >15 years were less likely to review, or review and upload, data onto NEHR. Doctors who regarded themselves as computer users with lower levels of technical aptitude and those who perceived an inadequate level of support were less likely to use the NEHR. The majority of GP had a positive attitude towards NEHR.
Conclusions: This study highlighted key demographics and perceived barriers affecting NEHR use. By raising awareness of these issues to policy makers and working to overcome these barriers, NEHR use may be increased.
INTRODUCTION
Electronic health records (EHR) are a consolidation of a patient’s entire health history and information, including inpatient hospitalisation records, outpatient clinic visits, laboratory results, imaging reports, and records of medication prescribed and dispensed. They allow for improved safety and co-ordination of care, resulting in better overall care for the patient and improved quality of documentation and administration efficiency.1 A centralised EHR can allow full interoperability and a seamless transmission of patients’ health information across different healthcare settings.2,3 Other advantages of EHR include enhanced clinical decision-making abilities and cost-effectiveness.4 There has been significant progress in EHR around the world5,6,7 with improved usability and increased usage. Yet, these systems have not been fully implemented and effectively utilised.8
Many studies have been performed to elucidate the barriers perceived by physicians and their approach to the adoption and usage of EHR.9-35 Several of these barriers are similar enough to be combined and categorised together to form several distinct domains, namely: organisation’s influence and control, adequacy of training, adequacy of support, personal factors, and ethico–legal issues.33-35 With regard to barriers involving organisation, these include the lack of administrator involvement in the physician’s implementation of EHR22,23 and an organisation’s control and supervision undermining a physician’s autonomy.24,33,34 Barriers regarding inadequacy of training include lack of and/or insufficient training13,17,33,34 and lack of sufficient assessments and feedback to ensure that users are proficient13 and competent trainers.14 Adequacy of support can be categorised as either technical or financial support. Specific technical support barriers include a lack of interoperability in supporting and migrating data from previous systems,9,17-20 unreliable technological support,14,20 and a lack of infrastructure for technical assistance.10,13,22 The financial barriers involve mainly the cost of implementation22-24 and EHR maintenance.20,21,24,30 Personal factors affecting the use of EHR include barriers pertaining to age,25,26 practice site,13,22 computer literacy and technical sophistication,9,11,21,27,28,35 and perceived negative effects on the patient–doctor relationship.18,19,33,34 Ethico–legal issues include breaches of security30-32 and compromised patient confidentiality.30-33
In Singapore, the National Electronic Health Record (NEHR) was launched in 2011, owned by the Ministry of Health (MOH) Singapore. The NEHR was developed and managed by Integrated Health Information Systems (IHiS), a technology agency for the public healthcare sector. The central ethos of NEHR was that of “One Patient, One Health Record”. The NEHR comprises a consolidated view of a patient’s healthcare history, including admission and visit history, hospital inpatient discharge summaries, laboratory results, medication history, history of past operations, allergies and adverse drug reactions, and immunisation history.36 By allowing a longitudinal view of the patient’s medical history, clinicians will be able to make better-informed diagnoses and treatment decisions, thus providing more effective and personalised care for patients and improving outcomes.
Registered physicians are allowed to access, review, and upload patient data. Anyone in Singapore, regardless of citizenship, who has been treated by an authorised healthcare professional from an institution or clinic that contributes data to NEHR will have a record. Singapore’s healthcare system consists of both public and private healthcare facilities and providers, with the former offering government subsidies for Singaporean people and permanent residents. As the provision of optimal care for patients requires a multidisciplinary team, including GP, specialists, therapists, and pharmacists, and often spans across public and private healthcare settings, a consolidated healthcare record will allow for holistic, comprehensive, and safe administration of care. Duplicative tests can be prevented, saving patients time and money. The patient experience will also be enhanced by a seamless continuity of care through transitions across different healthcare settings, for example from a GP clinic to a hospital. Sharing of critical patient information such as drug allergies will also significantly improve patient safety as the patient transfers across these various settings. In order to empower patients to take charge of their own health and improve self-maintenance health behaviours, they are also able to access part of their health records captured in the NEHR through a separate programme.37
A fund of 20 million Singapore dollars has been set aside to help private practices (including GP, private hospitals, private specialists, and dentists) offset the costs of updating their systems. MOH Singapore also intended to legislate a Healthcare Services Bill in 2018 requiring mandatory data contribution by all healthcare providers.38 Despite this, uptake has been slow, with an estimated 27% of private licensees in ambulatory care (GP, specialist, and dentists) accessing and reviewing NEHR and only 3% of them contributing and uploading data to NEHR (estimates from 01.01.2019).
The primary research objective of this study was to find out, amongst the private licensees, the actual proportion of GP who review patient data on NEHR, review and upload patient data to NEHR, and the proportion who have never used NEHR before. The secondary aim was to find out the characteristics of the GP in relation to their usage of NEHR (never use, review only, or review and upload), as well as identify the attitudes and perceptions (perceived barriers and facilitators) affecting their usage of NEHR.
METHODS
Study Design
This was an observational, cross-sectional, self-administered survey conducted in Singapore from 01.02.2018–31.07.2018 . A mailed survey was sent to a random sample of 523 GP working in clinics in the private sector, including doctors in both group (a chain of two or more clinics belonging to a single management) and solo practices. The self-administered questionnaire was addressed to the licensee of the clinic. Together with an introductory letter, the questionnaire and a return stamped envelope were mailed to a computer-generated random list of registered private GP clinics in Singapore. The survey was resent at 3 and 7 weeks after the initial mailing to those who had not replied, according to the Dillman protocol.39 To ensure that the data collected was anonymous to the investigators, an independent team oversaw the receiving and resending of the questionnaires to the nonrespondents. The study was approved by the SingHealth Centralised Institutional Review Board on 17.01.2018.
Survey Methods and Data Collection
The research instrument was a questionnaire developed using a combination of guidelines on authorship of surveys as well as previous research, review papers, and surveys on attitudes and perceptions of EHR and its perceived barriers.33-35 This questionnaire had been validated and tested for reliability in prior studies. Local contextual factors relating to Singapore were also taken into account.40 Questions on the managing organisation’s influence over physicians during the EHR preimplementation phase were excluded as these were irrelevant; the initiative had already been implemented nationwide in Singapore, compared to studies in which the EHR systems were still in the preimplementation phase.
This survey consisted of three sections. Section 1 elicited biodemographics of the participants and their self-reported computer literacy, using the terminology as adapted from previous surveys.33,34 Section 2 collected data regarding five domains, namely:
1) Adequate support.
2) Adequate training.
3) Physician autonomy.
4) Ethical and legal concerns.
5) Doctor–patient relationship.
A final section provided the respondents with an opportunity to provide comments. All questions, except those in the bio-demographics and comments sections, captured responses via a five-point Likert scale, ranging from “strongly disagree” to “strongly agree”. The final survey had been pilot-tested on an expert committee, consisting of senior family physicians as well as doctors within several hospitals’ informatics departments, ensuring face and content validity.
Statistical Analysis
Descriptive summary statistics (frequency and percentages) for the three categories of NEHR use (“never use”, “review only”, and “review and upload of patients’ data”), participant’s demographics, and the respective domains were computed. Multinomial logistics regression was performed to quantify the extent to which the NEHR use was affected by the participant’s demographics and the respective domains. The statistical analyses were performed using SPSS® Statistics 19 (IBM, Armonk, New York, USA).
Sample Size
Sample size was based on the assumed prevalence of NEHR use in Singapore, an estimated 50% out of a total number of 1,700 registered GP clinics in Singapore.41 With a confidence level of 95% and a margin of error of 5%, a sample size of 314 GP clinics was required.42 With the assumption of a 60% response rate,43 523 GP were surveyed.
RESULTS
There were 315 completed responses to the survey out of a total of 523 surveys sent, indicative of a 60.2% response rate. NEHR use was divided into the categories of “never use”, “review only”, and “review and upload”. In total, 74% of the doctors used NEHR for reviewing patient details, with 18% uploading data into NEHR; 8% of doctors surveyed had not used NEHR before. NEHR use amongst private GP for both review and review and upload of data was higher (74% and 18%, respectively) compared to all the private licensees in ambulatory care, specifically GP, specialists, and dentists (27% and 3%, respectively). Thirty eight percent of the respondents were females and 62% were males. Out of the 315 GP, 57% practised in a group practice and 43% were solo practitioners. The majority of the survey participants were aged 30–49 (30–39: 31.1%; 40–49: 47.9%). Fourteen percent were aged 50–59 and 7.0% were aged ≥60. Most of the GP had at least 11 or more years of experience (11–15 years in practice: 40.6%; >15 years in practice: 35.9%). In terms of personal computer or electronic device use, 92% of GP used their computers or electronic devices to access patients’ medical information; 92% used it to access email; 84% used it to access health and clinical resources such as journals; and 97% used the computer to surf the internet. The most frequent task the computer was used to perform in the clinic was patient registration (81%) and electronic documentation of patient consultation (82%), followed by the checking of results (78%), ordering of medications (76%), billing of patients (71%), and ordering of investigations (61%). A total of 47% of survey participants regarded themselves as general computer users, whereby ‘general’ was defined as ‘starting to become well-rounded and knowledgeable (in computers)’; 27% regarded themselves as ‘novice’ (‘a beginner with limited skills and privileges’) and 16% regarded themselves as a ‘technician’ (‘an advanced beginner; dabbler; starting to function creatively and assist others, but without significant expertise’). Approximately 10% of the participants considered their computer sophistication as ‘advanced’ (‘experienced, able to assist others independently and critically, and had usually completed formal training in computer science, medical informatics, or a related area’). No-one was an ‘expert’ (‘extra-seasoned; experienced; the most accomplished in the field; will have completed advanced training in both medicine and medical informatics or a related area’). The above points are summarised in Table 1.

Table 1: Summary of results regarding demographics.
*Definition of level of a computer user
Novice: beginner with limited skills and privileges; Technician: advanced beginner, dabbler, or starting to function creatively and assist others but without significant expertise; General: starting to become well-rounded and knowledgeable (in computers); Advanced: experienced, able to assist others independently and critically, will usually have completed formal training in computer science, medical informatics, or a related area.
Of the GP surveyed, 80.8% were worried that their autonomy would be affected, and that NEHR usage would excessively “increase control and monitoring of their clinical practices and decision-making.” Other barriers included concerns over ethical and legal aspects (62.6%), lack of technical support (61.0%), and cost of setting up and maintaining clinic NEHR access (51.0%). Nonetheless, 84.0% of GP felt that all physicians should “learn to use NEHR effectively”, and that “implementation of the NEHR technology will support the physician in providing better patient care.” GP in group practices were more likely to review and upload to the NEHR compared to GP in solo practices. Males were also more likely to review and upload compared to females, and those aged <40 were more likely to upload compared to those aged ≥50 (p<0.001). GP who had practiced for <15 years were more likely to use NEHR to review patient data compared to GP who had practiced for >15 years.
In terms of an individual’s self-reported computer sophistication level, doctors who regarded themselves as novice, technician, and general computer users were less likely to review NEHR compared to advanced computer users (p<0.001). A doctor who was a novice computer user was also less likely to review and upload data onto NEHR compared to an advanced user (p<0.001). There was no association between computer/electronic device usage and NEHR use. The more worried that the GP were of there being no adequate technical and financial support, the less likely they were to review or review and upload onto NEHR (p<0.001). The more positive an attitude taken by GP towards NEHR, the more likely they were to use NEHR for review or review and upload.
For the domains of adequate training, physician autonomy, ethical and legal concerns, and doctor–patient relationship, no significant associations were found (Table 2).
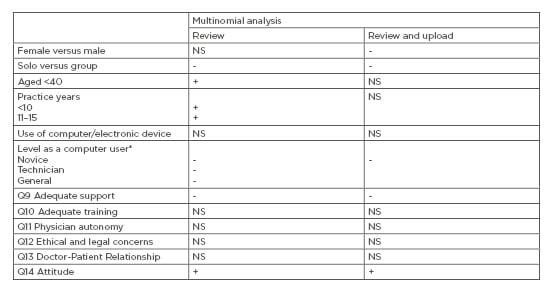
Table 2: Results of the study.
Only those p values that were significant were input as ‘-‘ or ‘+’, each denoting the respective direction of association with outcome.
*Definition of level of a computer user
Novice: beginner with limited skills and privileges; NS: nonsignificant; Technician: advanced beginner, dabbler, or starting to function creatively and assist others but without significant expertise; General: starting to become well-rounded and knowledgeable (in computers).
DISCUSSION
As this study was conducted nationwide across Singapore, the demographic data collected on age, years in practice, and computer experience was distributed across the different categories surveyed. However, it was noted that the majority of doctors surveyed had been practising for >5 years. This was likely secondary to the legislative requirements in Singapore for the setting up of a private medical practice. In Singapore, the MOH requires doctors to be fully registered before they can set up their own practices.44,45 Doctors who graduate from local universities are also bonded to the public sector for several years.46
In this study, GP in group practices were more likely to use the NEHR for review or review and upload of patients’ data, compared to solo practitioners. This result was similar to the conclusion reached by Xierali et al.,22 and may be attributable to better financial and resource support in group compared to solo practices.22 There may even be incentives and penalties, for usage and nonusage, respectively, of NEHR within the group. IT frameworks are most likely already set up and functional in these group practices. In addition, the doctors may be provided with IT training prior to joining the groups.
More GP who were <40 years old and had practised for <15 years were noted to review or review and upload data onto NEHR. This result was similar to a study by Kuek and Hakkenes,26 who postulated this difference to be because of education rather than the demographic variable of age. Younger doctors are more likely to have increased exposure to IT and may have received computer training during their school days. This information can be useful for policy makers, who can utilise this information to streamline and target promotion and training of NEHR use to this specific group of doctors, namely those in solo practice, who are >40 years old, and who have >15 years of experience in practice. This will allow better resource allocation.
As for the other barriers, doctors who regarded themselves as ‘general’ computer users tended to be more likely to use NEHR for review or review and upload of patient data compared to GP who considered themselves as ‘novice’ computer-users. This is similar to published results from a study by Alasmary et al.47 Again, this information may be useful for policy makers in conducting targeted computer training for these specific doctors as improving computer literacy and sophistication may improve use of digital information tools such as EHR.48 On a general level, policy makers can also work towards engaging the relevant IT partners to simplify the NEHR system for users. Doctors who perceived that there is inadequate support, both financially and technically, were also less likely to review or review and upload onto NEHR, results similar to many of the other studies done.10,13,20-22,24,30 This is in spite of a significant level of funding being channelled into NEHR implementation by the MOH Singapore.
From a financial perspective, the perceived inadequacy could be due to a lack of knowledge and awareness of the current available resources. Also, the current financial subsidies provided may still be inadequate, with GP requiring more funds to set up and maintain their computer system. From a technical perspective, the perceived inadequacy could include problems with contacting the computer personnel, the lack of support during after office hours, or even unclear instructions given to the doctors by the computer personnel.
This study is not without limitations. When assessing computer sophistication, it is important to note that self-reported scores are always subject to cultural and local influences and may not accurately reflect computer proficiency.49 Also, even though the questionnaire was addressed to the licensee of the clinic, the survey may have been delegated to another colleague to be answered, leading to response and selection bias. In terms of generalisability, this study was targeted towards GP in the private sector and hence the conclusions may not be applicable to primary care physicians in the public sector. This study explored GP perceptions of NEHR during the time frame indicated. As the emphasis of IT changes over time, with heightened awareness of cybersecurity50 and sustainable funding, perceptions and priorities may change.
Future research may include extending this study to primary care physicians in the public sectors and comparing both trends. On a wider scale, a recent survey on Singaporean people’s perceptions on NEHR51 revealed that most Singaporean people are generally supportive of NEHR as a tool to facilitate continuity of care as they move through the various healthcare settings. Their main concerns include patient confidentiality and data security. Future research can integrate and compare both the physicians’ and patients’ perspectives.
CONCLUSION
This first study of NEHR use in Singapore enumerated the actual proportion of GP who used NEHR. Through a detailed study of these GP, key characteristics associated with a reduced usage of NEHR were highlighted. These include solo GP who are >40 years old, those who have practised for >15 years, and those who regard their level of computer sophistication as novice. Amongst GP who were less likely to use NEHR for the purposes of reviewing or reviewing and uploading patient data, barriers were identified. These included a perceived inadequacy of technical and financial support. In general, the majority of GP were positive towards NEHR use in Singapore. GP with a positive attitude towards NEHR were also more likely to use it for reviewing or reviewing and uploading of patient data. By raising awareness of these issues to policy makers and working on these barriers, NEHR use may be increased.






