
Abstract
The importance of health literacy is well recognised. Health literacy has a strong impact on health status and is crucial for empowering patients to pursue a more active role in their own healthcare. Health information is one of the most frequently searched topics on the internet, and in the current networked environment, electronic health resources are becoming increasingly vital in improving overall health literacy. New technologies that allow a myriad of eHealth applications and communication channels are revolutionising the ways in which health information is accessed and used by both providers and patients. Hence, the concept of eHealth literacy, which is an individual’s ability to find, evaluate, and apply health information from electronic sources, is a crucial area of study to understand and enhance the ways in which patients access and use eHealth information. This study examines eHealth literacy levels among a group of UK baby boomers (individuals born between 1946 and 1964) (N=407) who had recently used the internet to search for health information. The results suggest that even among this group of internet users, there are skill gaps that need to be addressed before the full potential of these electronic resources in empowering patients to play an active role in their own healthcare can be reached.
INTRODUCTION
A woman, named Bernadette, collapses in a store and an ambulance is called. She does not regain consciousness until she is in hospital, where she becomes increasingly distressed. Hospitals and doctors terrify her. How will she cope in this alien environment, with forms to fill in, signs to read, and questions to answer? She cannot read or write very well; she left school aged 14 years because she fell pregnant, but had not attended much before that because she was looking after her younger siblings. She is worried about her husband’s reaction, too; they have been together for 50 years, how will he cope without her? It does not take long before the patient is diagnosed with ulcerating metastatic breast cancer and she dies a few weeks later, aged 64 years, having never sought any treatment prior to the day she collapsed in the store.
Bernadette’s story is true, but is not one that happened many years ago, or in a remote village in a developing country, it happened in one of the biggest cities in the UK in 2015. Bernadette’s story, though extreme, is not an isolated incident. Writing for NHS England, Berry1 tells of a woman who thought her ‘positive’ cancer diagnosis was a good thing; a man who, despite being directed to the radiology department many times, could not find the X-ray department, so went home; and a group of young women who did not know the location of the cervix in the body. These examples all have one thing in common: low levels of health literacy. Health literacy, defined as “the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand, and use information in ways which promote and maintain good health”,2 goes beyond being able to read labels or pamphlets, or make appointments; it incorporates tasks such as completing complex health forms, sharing medical history, seeking preventative healthcare, understanding the links between behaviour and health, and managing chronic health conditions.3,4 Health literacy is crucial to enabling people to actively improve and manage their own health. A body of research demonstrates that health literacy is a strong determinant of health status, with clear evidence that low health literacy is associated with poor health outcomes, including higher rates of hospitalisations and visits to doctors, lower rates of immunisations, and lower levels of health knowledge and understanding of health information.5,6
Vast amounts of health information and resources are available, and these are extremely valuable to those people who are health literate. Additionally, in today’s digital and networked environment, electronic health (eHealth) resources are revolutionising many aspects of healthcare and health promotion for both patients and providers. The World Health Organization (WHO) defines eHealth as “the cost-effective and secure use of information communication technologies (ICT) in support of health and health-related fields, including healthcare services, health surveillance, health literature, and health education, knowledge, and research.”7 Hence, there is now an additional dimension to overall health literacy: the concept of eHealth literacy, which is defined as “the ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to addressing or solving a health problem.”8 While overall health literacy has been investigated extensively, the relatively new concept of eHealth literacy remains understudied.9
This paper considers the levels of self-perceived eHealth literacy among a group of UK baby boomers (individuals born between 1946 and 1964) who were relatively health literate insofar as they had used the internet to search for health information in the previous 6 months. The paper begins with a brief overview of eHealth, before moving on to outline the importance of the baby boomer cohort from an eHealth literacy perspective. The details of the empirical study undertaken are described, before discussing the implications of the results for providers of eHealth resources.
eHEALTH
In many countries across the world, eHealth strategies are in various stages of planning and implementation. New technologies have delivered imaginative ideas, such as eHealth records, telehealth initiatives, mobile health-promoting applications, interactive health-related social media, and a myriad of online health information websites. Patients can now use electronic resources to book and change appointments, order prescriptions, access healthcare records, and interact with healthcare providers or other patients. There is also a vast array of health and wellbeing information on the internet, with websites providing details from general wellbeing facts to detailed information about diseases, treatments, and procedures. eHealth applications are often suggested as solutions to the consequences of ageing populations and the increasing prevalence of chronic diseases, combined with rising healthcare costs.10 Other promised benefits include enhanced quality of care11 and patient participation and empowerment, marking a shift as patients convert from passive recipients to active consumers of healthcare.12,13
The internet is a major source of health information,14 and over half of UK adults who use the internet have searched online for health information.15 However, it is difficult to imagine Bernadette, or people like her, searching various websites for insights about health issues. Bernadette was among many people who have insufficient levels of health literacy; nearly half of all Europeans have health literacy levels described as inadequate or problematic.16,17 In the UK, the available health information is too complex for 43% of working-age adults, a figure that rises to 61% if the information contains numbers,18 and the levels of inadequate eHealth literacy may be even greater. In 2017, almost 1 in 10 UK adults had never used the internet, and it has been shown that internet usage differs between sexes, with men displaying greater usage levels, and between regions, with London having higher internet usage than the rest of the UK. Notably, 22% of disabled people have never used the internet19 and, hence, a lot of health information is not useful for and/or not available among some groups in society.
Baby Boomers: Health and eHealth
Globally, life expectancy has increased by almost 20 years over five decades, leading the United Nations (UN) to describe population ageing as one of the greatest social, economic, and political transformations of all time.20 Ageing populations impact healthcare provision, and age-related diseases, such as cardiovascular disease, arthritis, osteoporosis, Type 2 diabetes mellitus, and dementia, place greater demands on healthcare providers. Indeed, while life expectancy has increased, overall morbidity rates have not changed; heart and respiratory disease, musculoskeletal problems, sensory impairment, diabetes (incorporating Type 1 and 2 diabetes mellitus), and depressive disorders remain the leading causes of morbidity in this cohort. Forty-five percent of the disease burden among baby boomers is attributable to lifestyle choices, such as poor diet, smoking, or being overweight.21
Nevertheless, many baby boomers are technologically skilled and increasingly taking a greater role in their own healthcare.22 Internet adoption is high among this cohort, with 90% of 55–64-year-olds and 78% of 65–74-year-olds having used the internet in the first 3 months of 2017. Notably, of those in the 55–64 year age cohort, half of individuals searched for health-related information;19 however, what is not fully understood is how fruitful these health-related information searches were. If eHealth resources are to reach their full potential, it is important to understand the levels of eHealth literacy among middle-aged adults, since this baby boomer cohort comprises the elderly of tomorrow, and, among older generations, low health literacy is associated with lower levels of health status, lower quality of life, and higher mortality.6,18
THE STUDY
Sample
Research Now Group, Inc., Plano, Texas, USA, a global leader in digital research data, was commissioned to administer an online questionnaire to a sample of baby boomers (born between 1946 and 1964). The questionnaire was sent to 3,000 randomly selected baby boomers and eligibility to participate in the study was dependent on having used the internet to search for health information in the last 6 months. The prospective respondents were informed of the questionnaire’s purpose (a research project studying the use of the internet to search for and share health information), academic nature, how the data would be stored (password-protected secure university files) and for how long, and the length of the survey, which typically took 20 minutes to complete. Since approximately half of the baby boomers used the internet to search for health information, the sample comprised early adopters of eHealth and the early majority23 in terms of acceptance of these technologies, and, as such, was expected to demonstrate relatively high levels of eHealth literacy compared to those who do not use the internet at all or those who do not use it for health-related information. The survey was open for 24 hours.
Health Literacy Measure
In addition to a range of questions pertaining to health and the eHealth resources used, the updated version24 of the eHealth Literacy Scale (eHEALS)8 was used to ascertain the levels of eHealth literacy among this sample of baby boomers. The scale has been used extensively in eHealth literacy studies around the world,25 and the objectives were defined as to “measure consumers’ combined knowledge, comfort, and perceived skills at finding, evaluating, and applying eHealth information to health problems”.8 The measure comprises eight items that together examine three distinct facets of eHealth literacy.24 The first facet measures the levels of awareness of what health resources and information are available on the internet; the second pertains to the skills and ability needed to find and use these health-related online resources; and the third reflects the individual’s self-belief and confidence that he or she can evaluate the different resources to use them effectively. These dimensions and the individual scale items are shown in Table 1.
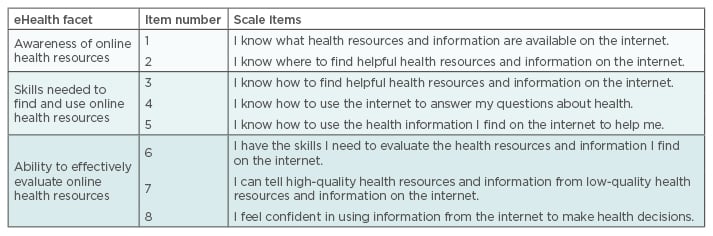
Table 1: eHealth Literacy Scale (eHEALS) measure.
eHealth: electronic health.
RESULTS AND DISCUSSION
A total of 407 responses were received. The mean age of the sample was 59.6 years and comprised 47% males and 53% females, with a variety of work statuses (for example, 48% were employed, 32% retired, 9% homemakers, and 9% unemployed), and levels of educational attainment (for example, 38.5% were educated to secondary school level, 36.5% to college, technical, or occupational level, and 24% had a degree).
Respondents reported an assortment of chronic health conditions, with over one-quarter of individuals suffering from hypertension and high cholesterol, almost 1 in 5 suffering arthritis, and around 15% reporting neural or mental issues, lung problems, or diabetes. One-third of the sample reported other chronic health conditions, with cancer, stroke, heart disease, fibromyalgia, and osteoporosis among the most common. When comparing the prevalence of chronic health conditions in this sample with the figures available in the public health domain,21 the sample of baby boomers investigated in this study are healthier than the wider population of baby boomers. Nevertheless, significant numbers are living with at least one chronic condition and many of these conditions, such as hypertension and high cholesterol, are often associated with unhealthy lifestyles.26 The economic burden resulting from such chronic diseases in these large numbers cannot be ignored, and preventative measures need to be given priority in healthcare.27
As shown in Figure 1, government-run specialist websites, such as NHS Choices, are the preferred choice for baby boomers when searching for online health information, with 45% using such sites regularly and a further 32% accessing them sometimes. Only 16% used general information sites, such as Wikipedia, on a regular basis, with over one-third turning to them occasionally. Online support groups and forums (such as cancer support and chronic obstructive pulmonary disease [COPD] support) were used at least occasionally by 38% and 23%, respectively, while other sources, such as blogs, electronic newsletters, and social media, were used less frequently and, for the vast majority of respondents, were never used. Therefore, the potential benefits of interactive social media, such as enabling individuals to become health advocates and collaborators,12 have some way to go before being recognised. Despite increasing adoption rates among older adults, young people are still the most likely to use social media,28 and, hence, these results may be less pronounced among younger samples. Nevertheless, these findings reflect results from earlier studies which report that, in comparison to using other internet health resources, the use of social media is lacking.29 Extensive research into social media with a health focus is still needed, and this is a topic for future research.30
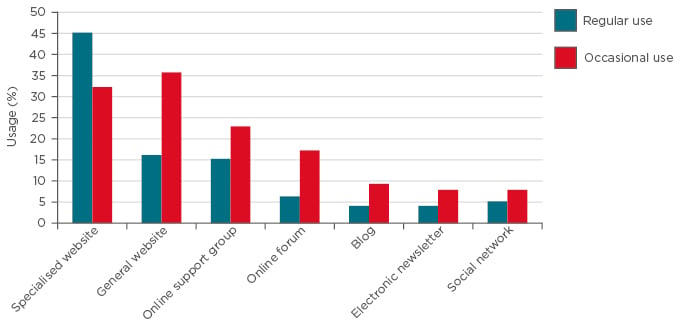
Figure 1: Sources of electronic health resources.
Even at this stage in the lives of the study participants, there is the potential for intervention to reduce modifiable risk factors.21,26 While the major information sources depicted in Figure 1 currently offer lifestyle information on diet and exercise, there is an opportunity for these key information providers to better stress preventative measures and the need for lifestyle changes. Perhaps the baby boomers who do not access such online resources are more important to consider and target education to. There is a very real risk of a ‘digital divide’,31,32 where health inequalities may be intensified as increasing numbers of health systems and health information rely on technology.
Turning to eHealth literacy, Figure 2 demonstrates the three elements and the average score for each of the eight items. The study sample comprised baby boomers who had used the internet to search for health information in the previous 6 months. Hence, the sample is drawn from the upper level of the cohort in terms of those who use the internet for eHealth purposes. There are still some discrepancies, however, in the levels of awareness of exactly what eHealth resources are available online (items 1 and 2). Given the nature of the sample, these baby boomers demonstrated relatively high levels of internet searching skills and, therefore, the majority felt confident that they knew how to find eHealth online resources (items 3 and 4). However, although the sample participants were relatively confident in terms of eHealth awareness and internet search skills, they were far less confident in their ability to effectively evaluate online health resources (item 6) (Figure 2). They also experienced difficulties in determining high-quality health resources and information from low-quality health resources and information on the internet (item 7) and did not feel particularly confident in using the online information they found to make health decisions (item 8). Concerns relating to the lack of control over the quality of some online health resources have previously been raised,12 and the fact that there are such high levels of evaluation problems, even among those who do use the internet for health information, is a major issue that needs to be addressed.
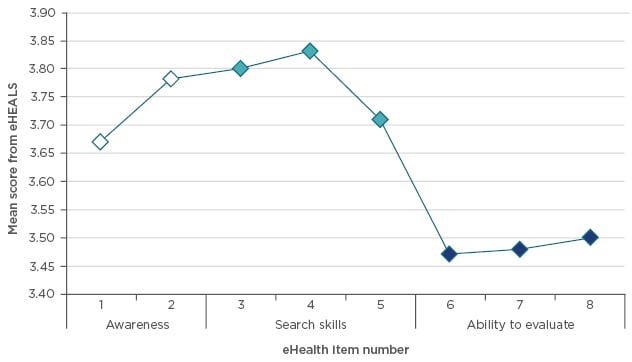
Figure 2: Electronic health literacy.
eHEALS assesses self-perceptions of three important and distinct (though inter-related) elements of eHealth literacy: Awareness of internet health resources (items 1 and 2), the skills needed to access them (items 3–5), and the self-belief that one can effectively evaluate them (items 6–8).24 See Table 1.
eHEALS: eHealth literacy scale; eHealth: electronic health.
Analysis was then used to examine differences within the sample. An independent t-test revealed highly significant differences between sexes (t=-5.508; degrees of freedom=405; p<0.001), with males demonstrating higher levels of eHealth literacy than females. There were no significant differences between those who worked and those who were retired or homemakers. However, the small number of unemployed individuals in this sample demonstrated significantly poorer eHealth skills than the rest of the sample (F(3,392)=1.778; p<0.05). Finally, a significant positive correlation was found between educational attainment and eHealth literacy (r=0.162; N=407; p=0.001). Most of these findings reflect the patterns identified in studies of inequalities among older people and overall health literacy. There is powerful evidence of gender inequalities in financial security in later life,33 and it is well established that people with limited resources, both financial and social, and low educational attainment are more likely to have restricted health literacy.34 The results found here suggest that eHealth literacy follows a similar trajectory. The one unexpected finding is the lack of significant differences between workers, retirees, and homemakers; however, it should be kept in mind that the term homemaker incorporates both traditional housewives, who are often female, as well as a growing number of older males who, for various reasons, are not actively seeking work and therefore not classified as unemployed.35 More research is needed in this area.
Clearly, even among these adopters of eHealth online resources, there is still a great deal of variance in the knowledge about the resources that are available, and there are particular skill gaps in the ability to evaluate and use this information to make informed health decisions. There are also differences within this sample, with lower levels of eHealth literacy found among women and less educated individuals. Therefore, there is a need to pinpoint the precise skill gaps and underlying reasons to allow effective design of training programmes to ensure that the vast array of online health resources are accessible and of value to this important cohort.
Perhaps what is even more important are those baby boomers who did not meet the criteria for inclusion in this sample. It is currently estimated that almost 90% of baby boomers use the internet, and half of these do so for health purposes.19 Clearly, this leaves 1 in 10 who do not have any access to these resources, and half of those baby boomers who do have internet access choose not to use online health resources. The vast amounts of online health information and lifestyle advice is failing to reach the majority of baby boomers.
This study is not without its limitations. First, it is a cross-sectional study, relying on a single-age cohort, and results may differ if a wider age range was used. Second, the study focusses solely on eHEALS, the most extensively used self-perceived measure of eHealth literacy,24 and does not include any objective measures. There are two previous studies that examined the relationship of eHEALS with actual eHealth literacy. In the first, 88 participants completed a variety of health-related performance tests to measure their internet skills.36 Results revealed no correlation between performance and self-perceived eHealth literacy as measured by the eHEALS scale. Therefore, this outcome cast some doubt on the validity of the eHEALS scale. A more recent study, however, finding this result “somewhat surprising”, used 15 computerised simulation tasks and compared the performance on these tasks to the scores on the eHEALS scale.37 In this second study, a correlation between self-perceived and actual eHealth literacy was found, though to a moderate degree, leading the authors to conclude that people make a reasonable evaluation of their eHealth literacy level, although not always accurately. More research needs to be conducted into the validity of the eHEALS scale as a measure of eHealth literacy.
CONCLUSION
Baby boomers are the elderly population of tomorrow and are forecast to place significant financial burden on healthcare systems.38,39 This sample was drawn from those boomers who use the internet for health purposes and so the participants were expected to demonstrate much more competent eHealth literacy skills than those boomers, currently >50% of this cohort, who do not use the internet for health purposes. Yet, even among this sample, there are skill gaps, particularly around evaluation and use of online health resources, and significant differences based on sex, work status, and educational attainment. Greater skill gaps could be expected within other samples of baby boomers and, hence, there is a need to address these gaps. Practical intervention and training in eHealth is crucial because eHealth has the potential to assist patients with chronic health conditions in self-management,40 which could significantly reduce the burden on healthcare provision. Improvements in competence levels of eHealth literacy will also have associated benefits in terms of confidence in using other eHealth resources, including eHealth records, patient portals, and self-management tools.41 Therefore, an understanding of the current skill levels and training gaps is needed for policy makers and healthcare providers to develop targeted interventions and training for different sectors of the population. This study suggests progression is needed before eHealth technologies can reach their full potential in empowering patients to play an active role in their own healthcare.






