BACKGROUND AND AIMS
Monitoring antibiotic consumption is a key part of the strategy to fight antibiotic resistance, one of the major threats to global public health.1,2 In France, general practitioners (GP) are responsible forthree-quarters of antibiotic prescriptions(AP).3 Given that prescribing behavioursrepresent one of the major determinantsin this resistance emergence,4 RegionalCenters of Antibiotic Therapy have been progressively set up since 2022 to support antibiotic prescribing, education, andantibiotic consumption monitoring. The study aimed to describe GPs’ antibiotic prescribing practices in one French region with one of the lowest GP densities and identify factors associated with high prescribing rates.
MATERIALS AND METHODS
A cross-sectional study was conducted using the French National Health Data System (SNDS), which contains all comprehensive information on healthcare consumption for approximately 99% of the French population, covering both outpatient and inpatient care.5 GP consultations in primary care practices in the Centre-Val de Loire region in 2023–2024 were extracted. For each practitioner, the proportion of consultations resulting in systemic AP was estimated based on the dispensation codes (J01 ATC) and GPs were categorised as high-volume prescribers if >3rd quartile (11.5%; median 8.5%). GP features and practice population (patient characteristics attributed to each GP) associated with higher AP were estimated through a multivariable logistic regression model.
RESULTS
Over the 2-year period, 1,936 GPs (55.5% men; average age: 52.9±12.9 years) prescribed antibiotics in 10.1% of the 15 million consultations provided to 4 million patients (24.6% of patients). Concerning GPs, over two-thirds had 5 or more years of professional clinical experience (71%; 35.8% ≥20 years), and 59.8% were located ≥5 km from an emergency department (31.4% ≥15 km).
Regarding patients, 44.9% were men, 8.0% were under 6 years old, 23.5% had a chronic disease and/or disability, and 10.3% were in a precarious situation. Regarding prescriptions, antibiotics accounted for 10.1% of consultations concerning 24.6% of patients.
The main prescriptions were amoxicillin (41.3%), macrolides (17.2%), and amoxicillin + clavulanic acid (14.5%). One quarter of GPs were high prescribers (n=491; 25.4%).
Factors associated with high prescription rates were linked to (a) patient population: young children (OR: 1.8 [95% CI: 1.3–2.5]), large male population >40% (3.3 [2.1–5.1]), socioeconomic deprivation (1.5 [1.2–2.0]), and fewer chronic diseases/disability (1.8 [1.4–2.4]; and (b) GP profile: ≥5 years’ experience with an increasing gradient (4.3 [3.1–5.9] if ≥20 years’ experience), emergency department ≥5 km with increasing gradient (1.6 [1.2–2.1] if ≥15km), GP practice in a socially deprived area (1.5 [1.2–2.0]), and practice department; whereas GP gender and access were not significantly associated to higher AP (Figure 1).
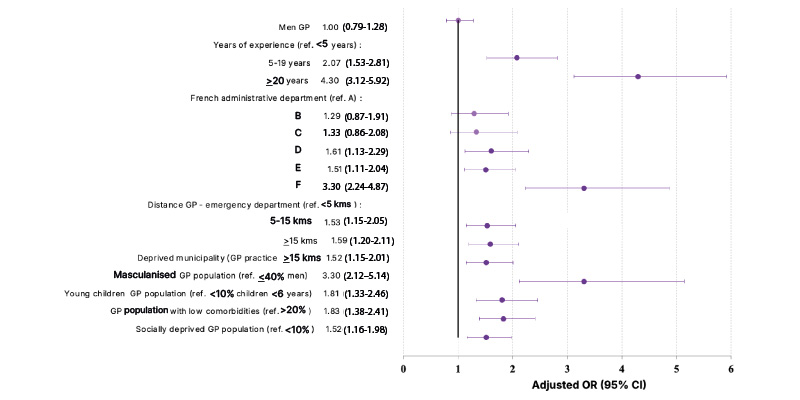
Figure 1: GP and patient population factors associated with being a major prescriber in Centre-Val de Loire, France, 2023–2024.
GP: general practitioner; OR: odds ratio; ref: reference.
CONCLUSION
This large-scale study pinpoints GP and patient factors driving higher AP, highlighting the importance of targeted interventions to promote antibiotic stewardship to tackle antimicrobial resistance.
Real-world data obtained via the SNDS can provide actionable insights for Regional Centers of Antibiotic Therapy, supporting intervention initiatives and informing public health strategies. However, further analyses will be required to identify more accurate prescription behaviours according to spectrum, duration, and adequacy of prescription/diagnosis.




