
INTRODUCTION AND AIMS
Adequate dialysis, as measured by Kt/V, is important for maintaining good health in haemodialysis (HD) patients. Guidelines recommend single pool Kt/V >1.2 as the minimum dose for thrice weekly HD.1 Despite a high regional prevalence of risk factors for chronic kidney disease and having a growing dialysis population,2 little is known about dialysis adequacy in the Gulf Cooperation Council (GCC) countries of Bahrain, Kuwait, Oman, Qatar, Saudi Arabia (KSA), and United Arab Emirates (UAE). Utilising data from the Dialysis Outcomes and Practice Patterns Study (DOPPS) from 2012–2018, this presentation describes: (1) a prevalence of low Kt/V (<1.2) in GCC countries compared to other international regions; (2) predictors of low Kt/V; (3) a relationship between low Kt/V and mortality; and (4) a percentage of low Kt/V cases attributed to treatment time (TT) and blood flow rate (BFR) in different patient subgroups.
METHODS
Data were acquired from initial cross-sections of the DOPPS 5 (2012–2015) and 6 (2015–2018) HD patients (N=1,544) on dialysis >180 days at 40 randomly selected GCC HD units. Country-level results were weighted for the sampling fraction in each unit. Logistic regression was used to estimate the proportion of low Kt/V cases attributable to various treatment practices, and multivariable Cox regression was used to estimate hazard ratios (HR) for low Kt/V on all-cause mortality with adjustments for numerous patient characteristics.
RESULTS
GCC HD patients had a mean age of 55 years, 41% were female, and there was a median dialysis vintage of 2.7 years. Mean BMI was lower for men compared to women (26.1 versus 27.5), but mean body surface area was higher for men compared to women (1.80 m2 versus 1.67 m2). GCC HD patients had the highest proportion of patients with single pool Kt/V <1.2 (34% versus 14%, 13%, 9%, and 5% in Canada, Japan, Europe, and USA, respectively). Kt/V was <1.2 in 27% of GCC females, versus 39% in GCC males. In multivariable logistic models, low Kt/V was more commonly associated (p<0.05) with larger body weight and height, male sex, lower TT, lower BFR, greater comorbidity burden, and use of HD as opposed to haemodiafiltration. BFR <350 mL/min and TT <4 hours were common (80% and 43% of patients, respectively). Men had higher mean BFR than women (306 mL/min versus 293 mL/min), and were less likely to have BFR <300 (25% versus 34%). In GCC patients, low Kt/V <1.2 was strongly related to higher mortality in women (HR: 1.86; 95% confidence interval [CI]: 1.11–3.14), whereas a weak mortality association was seen in men. If TT is increased to 4 hours and BFR is increased to 350, the proportion of low Kt/V would fall by 43% among patients with either low TT or BFR, and by 41% in all patients. Among females, 52% of all low Kt/V cases would increase to a Kt/V ≥1.2 if both TT and BFR were increased to target levels, while among males, only 36% of all low Kt/V cases would increase to a Kt/V ≥1.2.
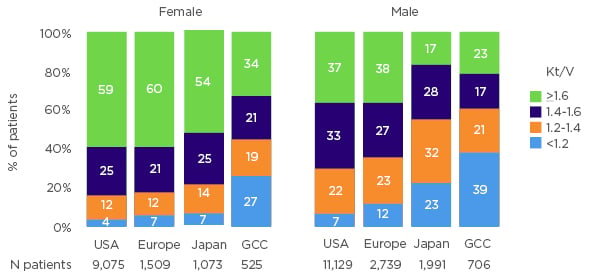
Figure 1: International comparison of Kt/V
Restricted to initial sample of patients at start of DOPPS 5 and 6, representing a prevalent cross-section. Countries included from Europe are Belgium, Germany, Italy, Spain, Sweden, and the UK. GCC: Gulf Cooperation Council; UK: United Kingdom; USA: United States of America.
CONCLUSIONS
Mean Kt/V was lower for GCC patients than all other DOPPS regions, with males displaying lower mean Kt/V than females in all areas. Low Kt/V appears related in part to short TT and low BFR, and may increase mortality rates, especially in females. Increasing BFR to 350 mL/min and TT to 4 hours thrice weekly in HD patients will improve Kt/V values and may further improve survival in the GCC, particularly for female HD patients.





