Abstract
Emphysematous pyelonephritis (EPN) constitutes a rare, gas-producing necrotising infection of the kidney. It primarily occurs in individuals with uncontrolled diabetes. It is mostly caused by Gram-negative Enterobacteriaceae like Escherichia coli or Klebsiella pneumoniae. Here, the authors report an unusual case of EPN due to Enterococcus species in a 56-year-old woman with diabetes who displayed symptoms suggestive of acute pancreatitis. Symptoms included epigastric and right upper quadrant pain, vomiting, and diarrhoea. Initial clinical and biochemical evaluation supported a diagnosis of acute pancreatitis, which was complicated by sepsis and acute kidney injury. A contrast-enhanced CT scan was performed as part of routine evaluation for pancreatitis severity and it incidentally revealed intrarenal gas consistent with EPN. Urine culture confirmed Enterococcus species. The individual was managed conservatively with broad spectrum intravenous antibiotics initiated empirically and later tailored according to culture sensitivity, along with strict glycaemic control. Her renal function and inflammatory markers normalised, and she was discharged by Day 9 in stable condition. This case highlights the importance of considering concurrent intra-abdominal pathologies in patients with diabetes. The authors also highlight the utility of imaging in uncovering atypical infections. This case underscores the importance of a multidisciplinary approach in managing such complex medical presentations.
Key Points
1. This case highlights the need for broad differential diagnosis in patients with diabetes who present with abdominal pain, because multiple overlapping pathologies may coexist.2. This case report describes an unusual dual presentation of acute pancreatitis with incidental early-stage emphysematous pyelonephritis due to Enterococcus, i.e., a rare causative pathogen.
3. Early imaging and antibiotic therapy, guided by culture, can prevent complications and eliminate the need for surgical intervention in complex diabetic presentations.
INTRODUCTION
Emphysematous pyelonephritis (EPN) is a highly uncommon and fatal necrotising infection of the renal parenchyma.1-3 It is characterised by gas production within the renal tissues, collecting system, or perinephric space. It occurs in patients with poorly controlled diabetes and is typically caused by gas-producing Gram-negative bacilli, e.g., Escherichia coli, Klebsiella pneumoniae, and Proteus mirabilis. Prompt diagnosis and intervention are critical, because the condition carries high morbidity and mortality if left untreated.4-6
The classical presentation includes fever, flank pain, and pyuria, but atypical or overlapping clinical scenarios can complicate timely recognition in patients with diabetes and multiple comorbidities.3 The Enterococcus species is usually associated with uncomplicated urinary tract infections. They are rarely implicated in EPN and are infrequently reported in the literature as causative pathogens in this condition.7
The authors present a rare and challenging diagnostic case of EPN caused by Enterococcus spp. in a patient with poorly controlled Type 2 diabetes, who initially presented with signs and symptoms indicative of acute pancreatitis, acute kidney injury, and sepsis. Thorough diagnostic evaluation and imaging can aid in uncovering coexistent or unsuspected intra-abdominal infections.
CASE PRESENTATION
A 56-year-old woman presented to the Emergency Department with a 6-day history of epigastric and right upper quadrant abdominal pain, vomiting, and diarrhoea. The abdominal pain was of moderate-to-severe intensity, continuous in nature, and radiating to the back. Pain intensity was partially relieved by assuming a forward-bending posture. She reported a history of burning micturition and fever 2 weeks prior, suggestive of a urinary tract infection, which was managed symptomatically without documented investigations or antibiotic therapy, potentially predisposing her to the current condition. Her past medical history included Type 2 diabetes, hypertension, and hypothyroidism, but she was poorly compliant with her medications. On examination, she was conscious with a Glasgow Coma Scale (GCS) score of E4V5M6, febrile, and haemodynamically stable.8 Physical examination indicated reduced breath sounds in the right infra-scapular region without added sounds, and tenderness in the epigastric region without peritoneal signs. There were no focal neurological deficits.
Initial laboratory evaluation showed marked leukocytosis (total leukocyte count: 26,920 /mm³ with neutrophilia), elevated serum creatinine (2.5 mg/dL), and blood urea nitrogen (175 mg/dL). This indicated acute kidney injury (Kidney Disease Improving Global Outcomes [KDIGO] Stage 2). Urine output was closely monitored and remained preserved throughout the clinical course, consistent with a non-oliguric presentation. In addition to renal involvement, the patient was diagnosed with acute pancreatitis according to the Revised Atlanta Criteria, based on characteristic epigastric pain and significantly elevated pancreatic enzymes (serum amylase and lipase were 494 U/L and 2,316 U/L, respectively).9 Severity assessment indicated mild-to-moderate disease, as there was no evidence of persistent organ failure or local complications. A thorough aetiological evaluation excluded common causes, including alcohol use, gallstones, recent endoscopic retrograde cholangiopancreatography, and exposure to any offending medications. In this context, the aetiology remained idiopathic after exclusion of common causes (Table 1). Glycated haemoglobin was 13.9% and indicated poor glycaemic control; procalcitonin was markedly elevated (7.33 ng/mL) and suggested a systemic infection. The chest X-ray did not contribute significantly to findings, highlighting limitations of early bedside imaging. CT imaging was performed to assess the severity and aetiology of pancreatitis. It indicated peripancreatic fat stranding and incidentally also detected gas in the right renal parenchyma (Figure 1). This confirmed EPN Class 2 according to Huang and Tseng classification.2 Urinalysis showed glycosuria and pyuria; urine culture yielded Enterococcus species with a colony count of >10⁵ CFU/mL, consistent with significant bacteriuria and sensitive to linezolid, ampicillin, vancomycin, and teicoplanin (Table 2). Species-level identification could not be performed due to laboratory limitations. Blood cultures were obtained as part of the sepsis workup and showed no growth.
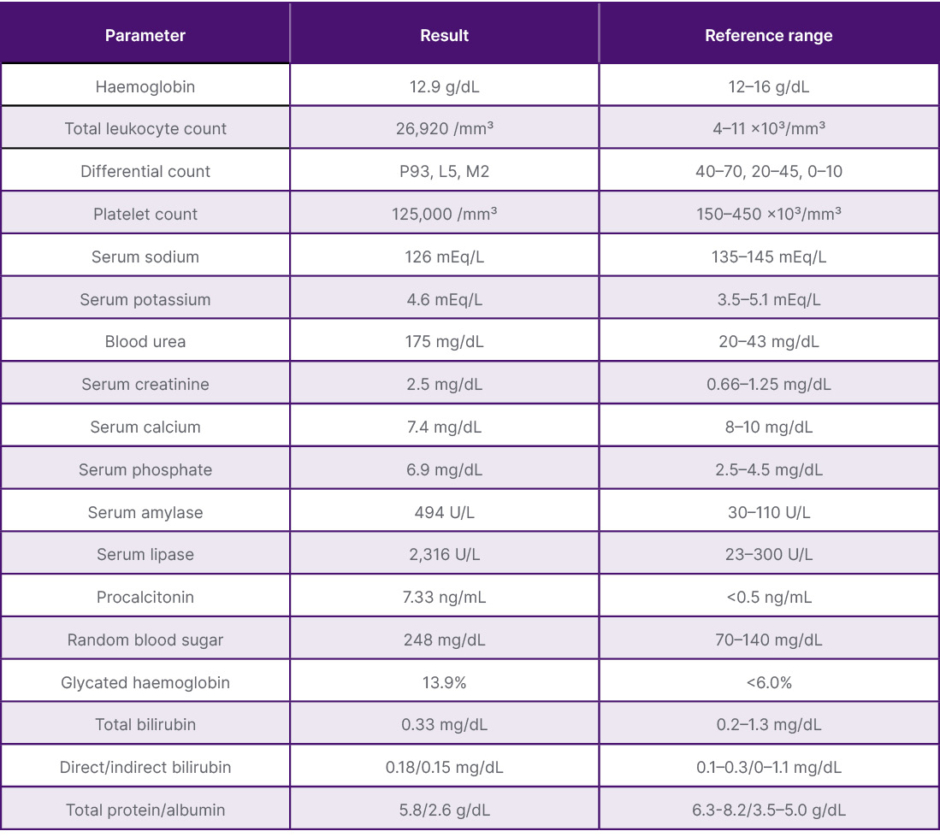
Table 1: Baseline laboratory parameters at presentation.
The initial evaluation summarised in this table is suggestive of severe bacterial sepsis complicated by acute kidney injury and acute pancreatitis, in the context of poorly controlled diabetes, accompanied by significant electrolyte disturbances, thrombocytopenia, and marked inflammatory dysregulation.
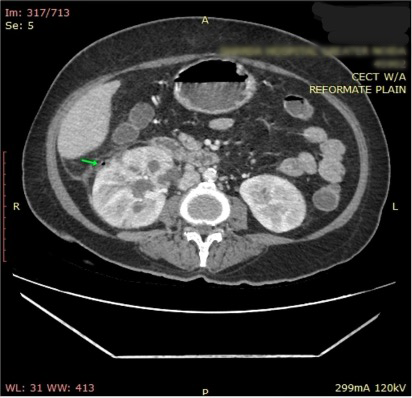
Figure 1: Contrast-enhanced CT abdomen showing Class 2 emphysematous pyelonephritis.
CT abdomen (axial view) showing peripherally enhancing collection with gas pocket in the right renal parenchyma and perinephric fat stranding, consistent with Class 2 emphysematous pyelonephritis according to Huang and Tseng classification.2
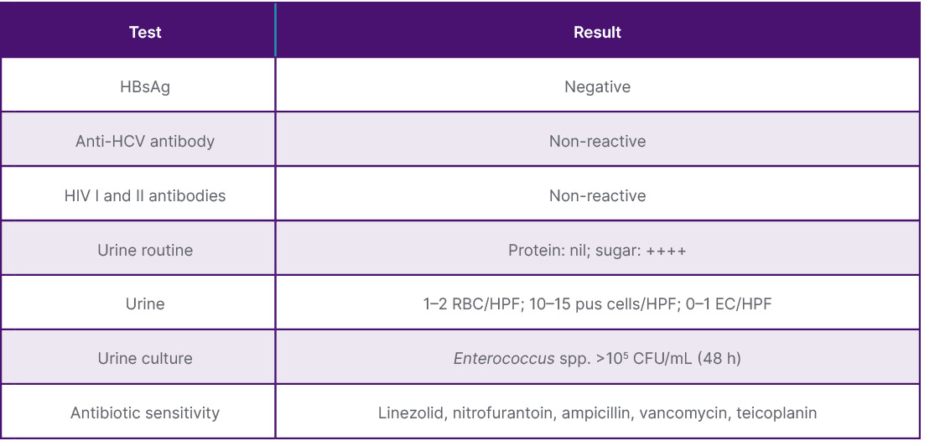
Table 2: Microbiological and serological investigations.
The patient exhibits negative serologies for HBsAg, anti-HCV, and HIV, while urine analysis demonstrates significant glycosuria and pyuria, with Enterococcus species bacteriuria confirmed by culture, superimposed on uncontrolled diabetes. EC: epithelial cells; HBsAg: hepatitis B surface antigen; HCV: hepatitis C virus; HPF: high-power field; RBC: red blood cells.
The patient was managed conservatively with a multidisciplinary approach. She was kept nil per oral initially with nasogastric decompression. Empirical therapy with piperacillin–tazobactam was initiated at a renal-adjusted dose of 2.25 g every 6 hours, and subsequently switched to intravenous ampicillin 2 g every 12 hours according to culture sensitivity, with dosing adjusted for renal function. This was then followed by oral linezolid. Glycaemic control was achieved with a basal-bolus insulin regimen, and thyroxine (75 μg once daily) was continued. Acute kidney injury was managed conservatively with intravenous fluids, strict input-output monitoring, and avoidance of nephrotoxic agents. Renal replacement therapy was not required. A soft, low-protein, low-fat oral diet was resumed on Day 5. By Day 9, the patient’s symptoms resolved and her laboratory parameters normalised. She was discharged in stable condition on oral linezolid 600 mg twice daily for 7 days, along with oral antidiabetic medications (oral linagliptin 5 mg once daily and oral metformin 500 mg twice daily) and thyroxine. At 4-week follow-up, the patient remained asymptomatic. Laboratory evaluation demonstrated complete normalisation of renal function, with serum creatinine returning to baseline levels. Glycaemic control was also maintained on standard oral antidiabetic therapy.
This case emphasises the importance of early imaging in patients with diabetes with abdominal pain, since it can uncover coexisting pathologies such as EPN, even in the absence of overt urinary symptoms.
DISCUSSION
The pathogenesis of EPN involves complex interactions between impaired host defences, high tissue glucose levels, and pathogenic bacterial metabolism.10,11 In uncontrolled diabetes, hyperglycaemia and worsened leukocyte function create a conducive environment for infection. Bacteria such as E. coli and K. pneumoniae produce gas via mixed acid fermentation of glucose and yield CO2 and hydrogen. These gases accumulate within the renal parenchyma and perinephric tissues. Enterococcus, however, is not a typical gas-forming organism, as it produces lactic acid via fermentation, generating minimal gas compared to typical organisms. Its presence in EPN has rarely been reported in the setting of hyperglycaemia and impaired tissue perfusion.12,13 Disease progression usually begins with focal parenchymal infection and can quickly evolve into diffuse necrosis and perinephric extension. Radiologically, this is indicated in the Huang and Tseng classification,2 which categorises disease based on the anatomical distribution and extent of gas within the renal parenchyma and adjacent structures. Severe forms are often associated with septic shock, multiorgan dysfunction, and high mortality. Early recognition and prompt intervention are therefore crucial, because progression from localised infection to widespread necrosis can occur within days in patients who are immunocompromised.
In the authors’ case, the patient was diagnosed with acute pancreatitis, sepsis, and acute kidney injury. It was during the radiological evaluation for pancreatitis that emphysematous changes in the right kidney were incidentally detected on CT, which demonstrated gas confined to the renal parenchyma without evidence of extrarenal extension, corresponding to Class 2 EPN. This is typically associated with a relatively favourable prognosis and is often amenable to conservative management. Imaging can aid in uncovering concurrent and clinically silent pathologies in high-risk patients. The patient’s initial presentation was severe, but timely initiation of broad-spectrum intravenous antibiotics, glycaemic control, and supportive care led to full clinical recovery without the need for surgical intervention or renal replacement therapy.14,15 The use of culture-directed therapy against Enterococcus spp. proved effective in this case.
In Class 2 EPN, literature supports that early-stage disease can often be managed conservatively: Somani et al.16 demonstrated successful outcomes with medical therapy alone, while Kapoor et al.17 and Chen et al.18 reported favourable survival in patients receiving antibiotics and supportive care. The classification-based approach described by Huang and Tseng2 further reinforces that patients with Class 1–2 EPN, in the absence of haemodynamic instability, may not require invasive intervention. The authors’ case exemplifies this principle, with complete resolution achieved through culture-directed antibiotics, glycaemic optimisation, and supportive care.
This case highlights the diagnostic challenges in patients with diabetes presenting with abdominal pain, where overlapping pathologies may coexist. The initial presentation suggested acute pancreatitis, but contrast-enhanced CT incidentally revealed early-stage EPN. Reports that describe the coexistence of EPN and acute pancreatitis are extremely limited in the literature. The involvement of Enterococcus as the aetiologic agent in EPN is even rarer. Minimal urinary symptoms and concurrent acute kidney injury further complicated timely recognition. Early imaging and culture-directed antibiotic therapy enabled successful conservative management, preventing progression and avoiding surgical intervention. This case adds to the limited body of evidence and supports conservative management in selected patients with early-stage or incidentally detected EPN, even in the presence of systemic complications.16,17 It indicates the importance of a combinative approach in the assessment and management of patients with diabetes who present with abdominal pain, e.g., when multiple intra-abdominal pathologies may coexist or may mimic each other. This rare combination is presented in the hope of raising clinical awareness and to promote early recognition and personalised management in such complex presentations.15






