BACKGROUND AND AIM
Gliomas are associated with variable survival, linked to their histological type.1 Although traditionally gliomas behave as if benign, low-grade gliomas (LGG) gradually evolve into high-grade tumours. Within 5 years, this will occur in approximately one-half of patients.2 The
diagnosis of LGG is challenging because conventional imaging modalities can often give inconclusive or equivocal results.3
Functional imaging modalities can provide additional metabolic information in the management of patients with LGG. O-(2 [18F]-fluoroethyl) -L-tyrosine (18F-FET) is a radiopharmaceutical approved for the characterisation of glioma-suggestive brain lesions.4-6
18F-FET displays a high tumour-to-background ratio and no accumulation in inflammatory lesions. Because of low uptake in normal brain parenchyma, some centres use fluoromethyl-(18F)-dimethyl-2-hydroxyethyl-ammonium chloride (18F-FCH) PET for the characterisation of glioma-suspected brain lesions. The aim of this study was to determine the diagnostic accuracy of 18F-FET and 18F-FCH PET/CT in patients with primary LGG.
METHODS
11 patients aged 21–80 years with MRI-suspected LGG were involved. Patients underwent both 18F-FET and 18F-FCH PET/CT within 1 week. Brain PET/CT was performed according to standard protocol: 20 min after intravenous injection of 185MBq of 18F-FET and 185MBq of 18F-FCH PET. Surgery and histological diagnoses were performed in the following 2 weeks.
All 11 patients with suspected LGG underwent MRI, 18F-FET, and 18F-FCH PET/CT. All patients had LGG according to MRI. In all PET-positive patients, tumour location on MRI was consistent with region of PET/CT positivity. Two out of 11 patients included in this study did not undergo surgery or biopsy for histological confirmation. Both had negative 18F-FET PET and negative 18F-FCH PET scan, so they declined surgery and multidisciplinary tumour board recommended follow-up. Nine out of 11 patients with suspected LGG had final histological diagnosis after the surgery.
RESULTS
The results of the study are summarised in Table 1. Significantly better concordance was described between tumour histology and 18F-FET PET results (weighted κ: 0.74) compared to both 18F-FCH (weighted κ: 0.15) and MRI results (weighted κ: 0.00). Significant association between tumour histology and 18F-FET results was found (odds ratio: 12.87; 95% confidence interval [CI]: 0.49–333.70; p=0.013, logistic regression analysis). Most patients with histologically-proven LGG had negative 18F-FCH and positive 18F-FET (Figure 1).
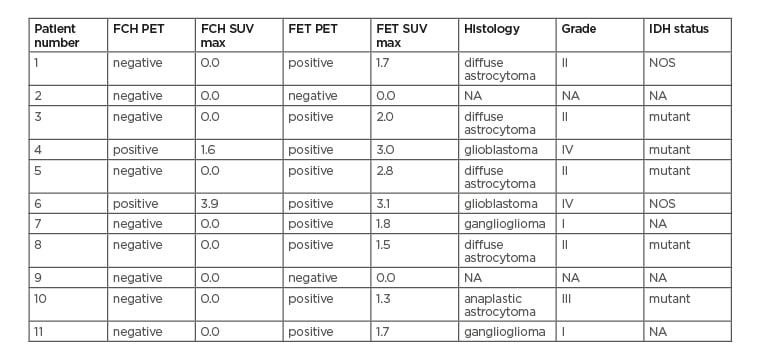
Table 1: Diagnostic workout of patients included in the study.
FCH: Fluoromethyl-(18F)-dimethyl-2-hydroxyethyl-ammonium chloride; FET: O- (2-[18F]-fluoroethyl) -L-tyrosine; IDH: isocitrate dehydrogenase; NA: not applicable; NOS: not otherwise specified; SUV max: maximum standard uptake value.
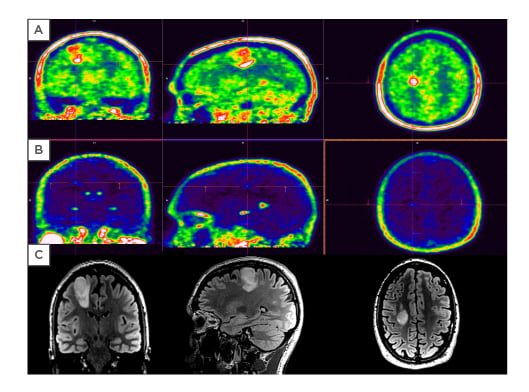
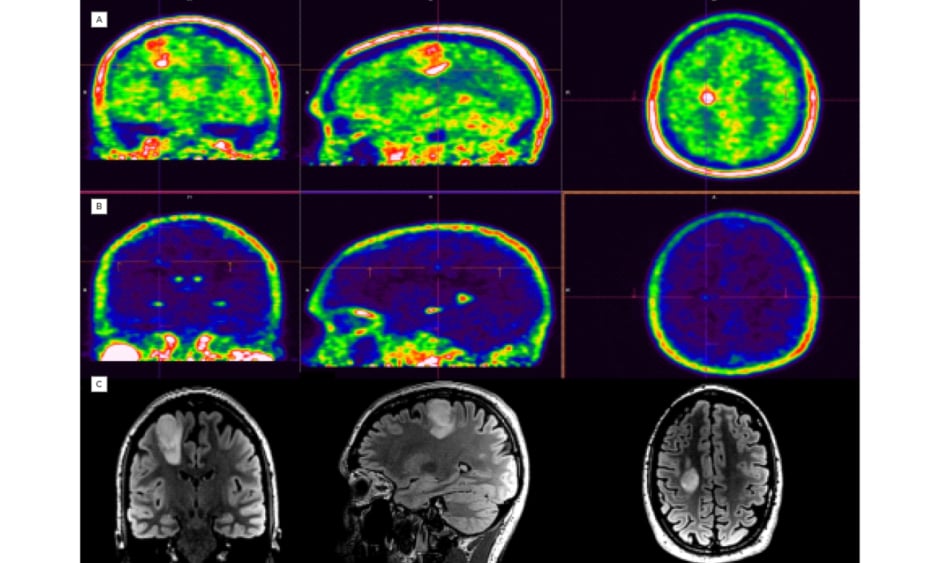
Figure 1: 38-year-old male patient with World Health Organization (WHO) Grade II diffuse astrocytoma.
A) positive 18F-FET PET/CT (SUV max: 2.8); B) negative 18F-FCH PET/CT; and C) MRI of a fast fluid-attenuated inversion recover tumour in right frontal lobe.
FCH: Fluoromethyl-(18F)-dimethyl-2-hydroxyethyl-ammonium chloride; FET: O-(2-[18F]-fluoroethyl)-L-tyrosine; SUV max: maximum standard uptake value.
CONCLUSION
These results demonstrate that the appropriate radiopharmaceutical should be chosen before performing PET/CT scan in patients with newly diagnosed LGG. The 18F-FET PET/CT is more accurate than 18F-FCH to detect LGG.






