Abstract
Objective: Describe CT and MRI features of the lymphoepithelial cyst (LEC) of the pancreas.
Methods: The authors identified 13 cases of LEC by searching their institutional electronic medical archives from 2004 to 2020. All of the patients had CT scans and six patients had both a CT and MRI. The final diagnosis was established either by fine-needle aspiration with cytopathology (n=6) or surgical resection (n=7).
Results: The mean diameter of the cysts was 36 mm (range: 6–93 mm). Almost all of the cysts were exophytic (92%) and solitary (85%), favouring the tail (54%) or body (38%) of the pancreas. LECs were either oval (62%) or round (39%) and had well-defined contours. All LECs showed T2 hyperintensity and T1 hypointensity; however, the signal was heterogeneous. Diffusion-weighted imaging showed restricted diffusion in all cases. On CT, LECs commonly showed complex fluid density (>15 HU) with no visible septation, enhancement or calcification.
Conclusion: LECs have a distinguishing feature on MRI, which is restricted diffusion on diffusion-weighted imaging. This is presumably secondary to the presence of keratin, which can be a helpful feature differentiating LECs from other pancreatic cystic neoplasms. Besides this, LECs predominantly appear as solitary and exophytic lesions, with complex fluid density on CT and heterogeneous hypointense T1 and heterogenous hyperintense T2 signal on MRI.
INTRODUCTION
As the list of cystic pancreatic lesions grows, so does the importance of accurate characterisation and recognition of the various entities that form this differential diagnosis. A lymphoepithelial cyst (LEC) is a rare benign lesion of the pancreas of uncertain pathogenesis that occurs almost exclusively in males.1 LECs comprise an important category in the differential diagnosis of cystic lesions of the pancreas. Histologically, these cysts contain keratin and are lined by mature stratified squamous epithelium surrounded by dense lymphoid tissue.2 The imaging appearance can mimic other cystic neoplasms; therefore, distinguishing LECs from other benign, premalignant, or malignant cystic lesions is important.
The radiology literature is limited to a small number of case series of CT and case reports of MRI of this entity.3,4 Definitive diagnosis has traditionally relied on histopathologic evaluation following resection. It is important to differentiate benign cysts from premalignant cysts to prevent unnecessary surgery.5 In this study, the imaging features of 13 cases of pancreatic LECs are presented and its differential diagnosis from other cystic lesions is discussed.
MATERIALS AND METHODS
Case Selection
Ethics Committee approval has been obtained. The institutional review board waived the requirement for obtaining a written consent form for this study. Radiology, gastroenterology, surgical, and cytology archives from 2004 to 2020 were searched retrospectively to identify patients with LEC. A total of 13 cases were identified and the diagnosis was established either by fine-needle aspiration (FNA) with cytopathology (n=6) or surgical resection (n=7).
Imaging Studies
A CT scan was performed on the multi-slice CT scanner, with post-contrast study after evaluating each patient’s serum creatinine and glomerular filtration rate. Approximately 100–120 mL of Isovue-370 and portal-venous phase (45–60 sec) scanning was performed from the dome of the diaphragm to pubic symphysis. An MRI was performed with basic T1-weighted, T2-weighted, T1-weighted in and out phase imaging, diffusion-weighted imaging (DWI) and apparent diffusion coefficient (ADC) map. DWI was used (b values used were 50, 400, and 800) and performed in 3T MRIs. The T1-weighted post-contrast phase of MRI study was performed in arterial, portal-venous, and delayed phases.
Image Data Collection
A fellowship-trained pancreas radiologist with 21 years of experience reviewed the imaging studies. The radiologist noted cyst location (head, body, or tail), size (in mm), exophytic or endophytic, shape (oval or round), and contour (smooth or lobulated). On CT images, CT density was measured in all cases. If the fluid was less than <15 HU, it was labelled as simple fluid and if it was >15 HU, was labelled as complex fluid. Presence of calcification and enhancement was noted. On MRI images, the radiologist recorded the presence of septations, T2-weighted signal (hyperintense or hypointense, homogenous or inhomogeneous), T1-weighted signal (hyperintense or hypointense, homogenous or inhomogeneous), and finally recorded the ADC signal (decreased, increased, or iso signal).
Histopathologic Evaluation
Cytology results were reviewed and confirmed by an experienced cytopathologist. The presence of nucleated and/or anucleated squamous cells. admixed with a variable number of lymphocytes on FNA smears, was considered diagnostic of LEC. In cases where FNA cytology was non-diagnostic, the diagnosis was established by a histopathologic evaluation of the surgical resections. The diagnosis was confirmed by surgery in seven cases, while the remaining cases were diagnosed by FNA cytology.
RESULTS
LECs were found in 12 males and 1 female, with a mean age of 56 years (Table 1). All patients had CT scans, and six patients had an MRI. The indication of the study included a pancreatic cyst in five patients, abdominal mass in three patients, abdominal pain in two patients, two evaluations of an incidental finding, and one for a liver lesion. These lesions were exophytic 92% of the time and predominantly located in the tail (54%), followed by the body (38%) and head (8%). The mean size was 36 mm (range: 8–94 mm). The shape was oval in 61% of cases and round in 39%. The contour of the cyst was smooth in 54% of cases, lobulated in 38%, and irregular in 8%.
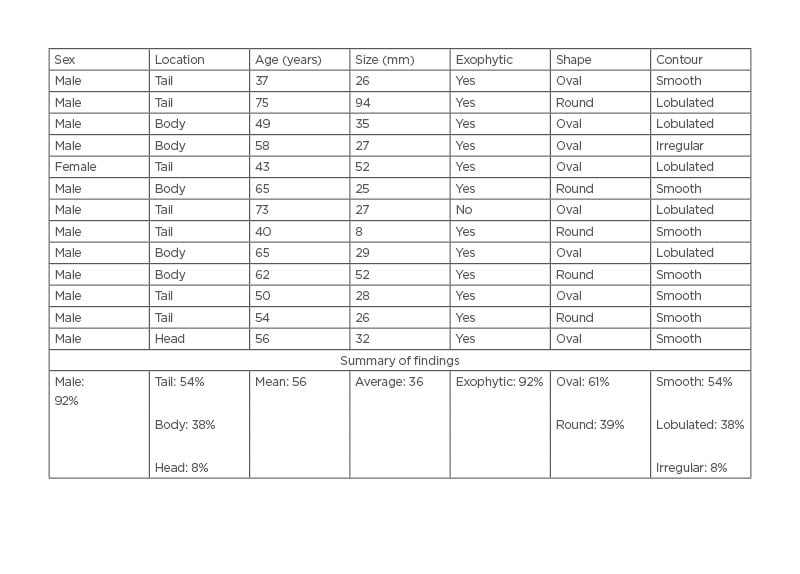
Table 1: Macroscopic features of lymphoepithelial cysts.
CT imaging features of LEC are listed in Table 2. There were no septations or enhancement in 92% of the cases (Figure 1). Most cases (62%) measured complex fluid (density: >15 HU). None of the cases showed calcification.
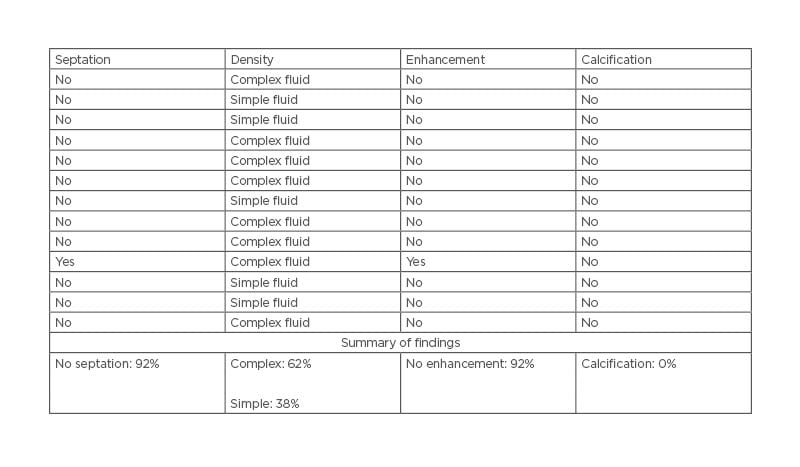
Table 2: CT imaging features of lymphoepithelial cysts.

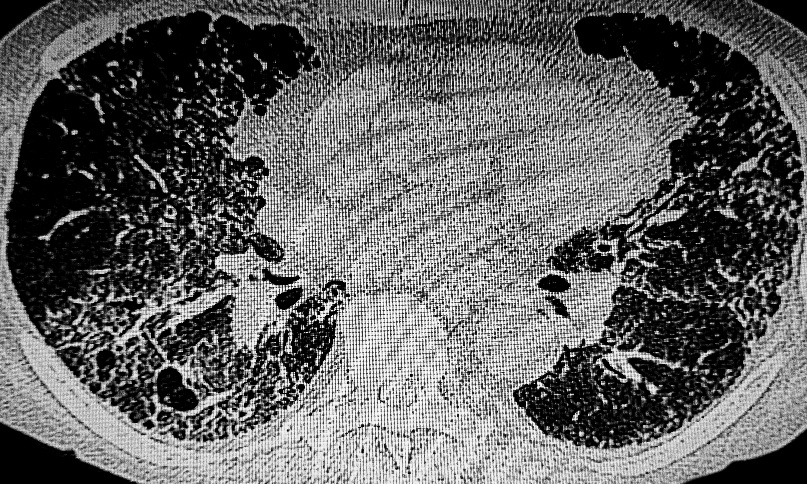
Figure 1: CT images of a lymphoepithelial cyst found in a 65-year-old male.
A) This is an axial contrast-enhanced CT image of an incidentally found LEC in a 65-year-old male. The cyst was oval, had sharply demarcated margins, and the CT density measured 32 HU (arrow). There are no visible internal septations or nodularity. B) This is a coronal reformat of the same cyst (arrow) and shows the exophytic location in the pancreatic head (P).
LEC: lymphoepithelial cyst; P: pancreas.
MRI features of LEC included T1, T2, internal septation, and ADC signal on DWI, which are listed in Table 3. All patients showed inhomogeneous hyperintense signal on T2-weight imaging and the majority (83%) showed inhomogeneous hypointense signal on T1-weighted imaging. Septations were seen in 50% of MR cases and were enhancing in two-thirds of cases. Diffusion restriction was seen in all three cases when the diffusion images were performed (Figure 2).
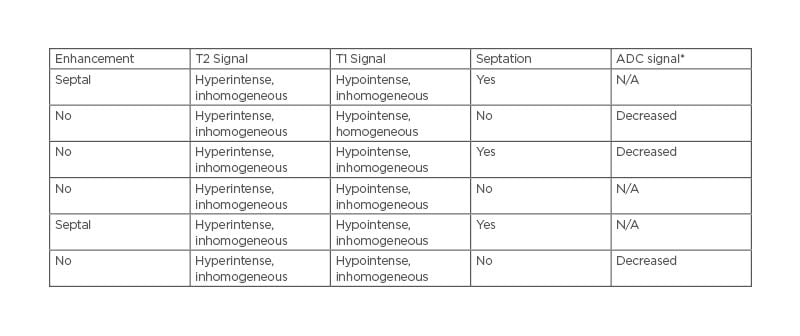
Table 3: MRI features of lymphoepithelial cysts.
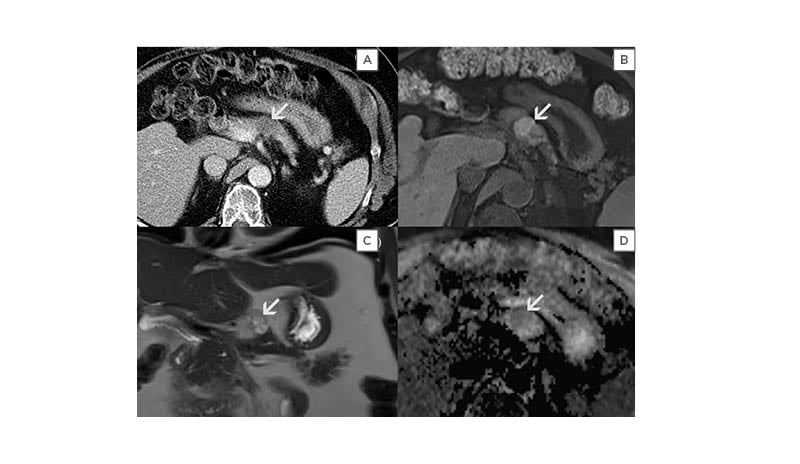
Figure 2: Diffusion restriction as seen three cases when diffusion-weight imaging was performed.
A) This is an incidentally found LEC seen in a 56-year-old male. An axial CT image with contrast showed an oval low-density lesion (arrow) in the pancreatic body. CT imaging features are non-specific; therefore, further evaluation with MRI was performed. B) This is an axial unenhanced T1-weighted image with fat suppression of the same cyst. There was a heterogeneously mixed signal intensity indicating complex nature of the cyst. C) This is a coronal T2-weighted image without contrast or fat suppression. LEC had septations and shows an inhomogeneous hyperintense T2 signal (arrow). D) This is an axial ADC map image of the same cyst in the pancreatic body (arrow). There is a hypointense signal that indicates restricted diffusion. This was presumably secondary to keratin content, seen with LECs, and is a useful differentiating feature from other pancreatic cystic neoplasms.
ADC: apparent diffusion coefficient; LEC: lymphoepithelial cyst.
DISCUSSION
A LEC is a rare but benign cyst of the pancreas.6 There are several hypotheses about histogenesis of the LEC, including squamous metaplasia of the pancreatic ducts with subsequent cystic transformation; ectopic pancreatic tissue included in a peripancreatic lymph node; epithelial remnants with peripancreatic lymph nodes; and ectopic remnants of a brachial cleft cyst that are misplaced and fused with the pancreas during embryogenesis.7,8 These cysts contain caseous, cheesy, or curd-like material and are lined by squamous epithelium containing keratin, surrounded by lymphoid tissue with rare follicles.2
The pathological diagnosis of a LEC is usually straightforward; however, the imaging features on CT or MRI are not well known. A LEC is a benign entity; therefore, if the imaging characteristics of a cystic pancreatic lesion are highly suggestive of a LEC, unnecessary surgery can be avoided.9
In the authors’ data series, LECs were predominantly seen in middle-aged males (mean age: 56), with a male to female ratio of 12:1. Yanagimoto et al.10 reviewed 106 cases of LECs, and the mean age of presentation was also 56 years, with a 4:1 male to female ratio. Most of the lesions in the authors’ study were located in the body or tail and were exophytic, similar to prior reports.11 Previous studies reported CT scan findings as a simple or complex cyst, septations, papillary projection, or solid component, which may enhance and wall calcification.12 However, in the authors’ case series, septations were seen in 50% of cases with MRI and 8% with CT. This discrepancy in septations is probably due to the insensitivity of CT in showing internal architecture (Figure 2). The authors measured complex fluid density in 62% by CT and inhomogeneous T1 and T2 signal in almost all cases.
The most distinguishing imaging feature of LEC was seen on DWI (Figure 2D). LECs showed restricted diffusion (i.e., hypointensity) in all three cases on the ADC map. This was probably due to the presence of keratinised material in these lesions and can be a useful distinguishing feature of LEC.13-15 This characteristic feature was also reported on prior case reports.4 T1-weighted images showed heterogeneous hypointensity in patients (five out of six) and T2-weighted images showed heterogeneous hyperintensity in all (six out of six) cases. Heterogeneous T1 and T2 signal are presumably due to the presence of cholesterol and keratin within the cyst.
The authors’ study was limited by the low population size. However, this is expected in rare cases such as LEC. There was not a big enough sample size to generate inter-observer variability using multiple readers.
In summary, a LEC is a rare, predominantly solitary, and exophytic lesion commonly found in the body or tail of the pancreas. On DWI imaging, all LECs showed restricted diffusion secondary to presence of keratin, which can be a distinguishing imaging feature from other pancreatic cystic neoplasms. Otherwise, CT and MRI findings are non-specific. They commonly showed complex fluid density on CT or heterogeneous hypointense T1 and heterogenous hyperintense T2 signal on MRI.