Prof Apostolos Karantanas | ESR Subspecialties and Allied Sciences Committee Chairperson Department of Medical Imaging, University Hospital, Heraklion, Greece Medical School-University of Crete, Heraklion, Greece Biomedical Laboratory, Institute of Computer Science, FORTH, Heraklion, Greece
![]()
Upon completing medical school in Greece, you went straight into radiology training; had you always known radiology would be your specialty of choice?
No, actually not. At the end of my undergraduate studies, in the early 80s, there was a robust social and political movement in favour of the rights of the patients with psychiatric disorders. Young people, and this is the right thing to do, are sensitive to human rights and of course to patients’ rights. This happened to me as well. Emotion took over realism and lifelong planning. However, when I was actively involved in psychiatry during the last year of my medical studies, I was disappointed in the results. Then, I had a short trip through focussing on ophthalmology, but soon I thought its scope was very narrow. I like the big picture. At this point, a good friend of mine, a young consultant in radiology, told me that radiology is the right path for those who like physics and experiments, and for those who are able to adapt to changes. There was neither PC nor internet at the time, of course. Soon, a cascade of events, including ultrasound, CT, interventional radiology, and informatics, starting within the first months of my training, showed me that I made the correct decision.
Having worked internationally in both the USA and the UK, could you tell us how radiology practice differs across the world and what you have learnt from your international experience?
In the USA, there is clearly as much infrastructure as required to practice updated radiology. There is also an orientation towards quality, safety, and excellence, which has been established over the decades among various scientific bodies. The USA is one of the countries most committed to setting high standards in clinical radiology globally, and to practice for the benefit of the patients. In the UK I really enjoyed, and learned a lot from, the clinical approach to patient problems. Funding is limited compared to the USA, but the existing technology is better used.
In my practice, as a musculoskeletal radiologist, I encourage my residents to meet and talk to the patients and I train them to get a complete history and make a basic clinical examination. Patients are capable of providing us with half the diagnosis.
You recently authored the paper ‘Diabetes: a silent player in musculoskeletal interventional radiology response’. What should radiologists and those in allied sciences be vigilant for regarding this topic?
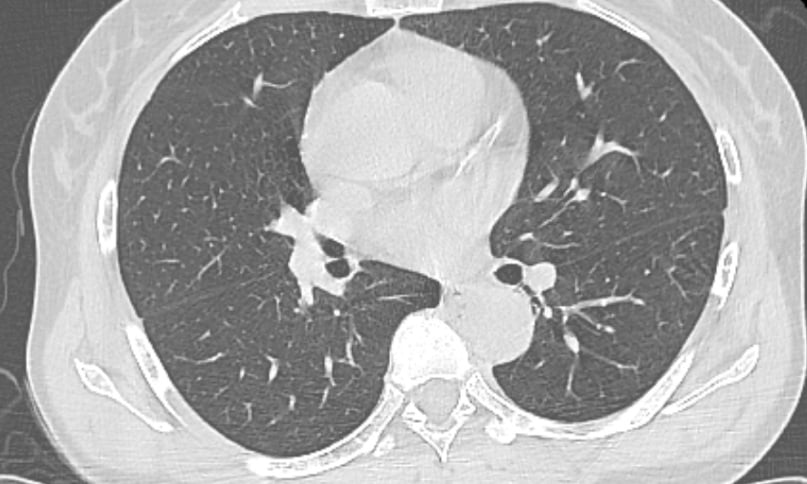
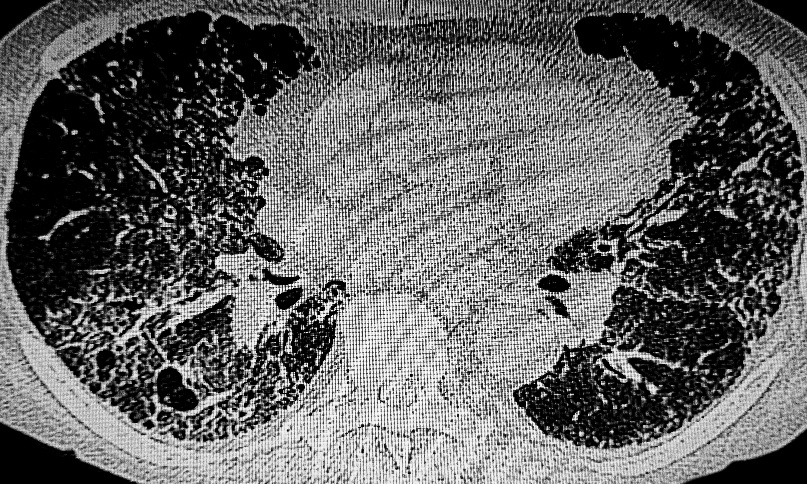
The paper was primarily authored by a young Portuguese radiologist, Sofia Dimitri-Pinheiro, who is conducting PhD under my supervision. We are doing a joined project, in two countries, Portugal and Greece, on the results of minimal invasive, ultrasound-guided treatment of adhesive capsulitis. Diabetes affects practically all organs and systems, with the musculoskeletal one being relatively spared up to now as regards literature reports. Recent research has shed light into the fact that diabetes has an important role in the development of several disorders, such as adhesive capsulitis of the glenohumeral joint, stenosing flexor tenosynovitis of the finger, and the very common calcific tendinopathy.
What do you hope to achieve in your role as ESR Subspecialties and Allied Sciences Committee (SASC) Chairperson?
I do not only hope but also plan to achieve several goals. The SASC has an important role, clearly defined by the ESR statuses. I have to act as a link between the ESR leadership and the presidents of all 15 ESR Subspecialty and Allied Sciences Societies as well as between the SASC and other relevant ESR bodies in order to facilitate co-operation and co-ordinate efforts. In addition, I advise the Executive Council on matters relevant to the subspecialties of radiology and allied disciplines and I assist the ECR Programme Planning Committee in the preparation of the educational and scientific programme.
Apart from the conventional duties, I have started an update of the hot topics of all subspecialty societies and I have invited them to nominate representative to the European Society of Medical Imaging Informatics (EuSOMII) because of the rapid development of AI in research, education, and clinical practice.
Last but not least, my main tasks will be: 1) the establishment of increased exposure of radiologists among clinicians and patients because of the invisibility that teleradiology has induced and 2) the establishment of curriculum and accreditation for forensic radiology, which is a rapidly expanding field that radiologists cannot ignore.
The ‘In Focus’ programme for ECR 2021 will focus on physical and mental wellbeing. Is this becoming a larger conversation in the medical profession?
Yes, indeed. If you visit the website of the National Health Service (NHS), UK, one of the main topics on the first page is ‘healthy living’, with tips and tools on the best choices about health and wellbeing. I totally agree with this perspective and a constant conversation on this issue goes on, among various medical professionals. This is also the case the other way around. Wellbeing, or good health status, is directly related to the public demand that physicians be fully aware of need for lifelong learning. Thus, one of the most important issues in this conversation is maintenance of certification and this is a matter of extensive discussion throughout the world.
Once a week, I offer a second opinion service for patients with musculoskeletal problems; these patients carry with them numerous imaging studies! In the vast majority of the visits, particularly during the pandemic which induces extra stress, the imaging findings do not match the subjective descriptions from the patients regarding their symptoms. In other words, the body looks healthy, but the subject feels and acts like a patient. Thus, healthy living is a wide umbrella which includes mental activity, body training, and psychological stability.
What are the key challenges that are faced by radiologists and those in allied sciences? And what approach would you recommend combatting such challenges?
Sherlock Holmes used to say on the obvious, yet for others obscure, events: “Elementary, my dear Watson.” Technological innovations are so quick that the only skill we, and particularly the younger radiologists, should have at the highest possible level is ‘open eyes’. In other words, ‘open mind’. Radiology now is part of an extended family. In our practice, we work very closely with medical physicists, mathematicians, informatics, advanced image analysis specialists, statisticians and more. Clinical radiologists provide the data and the ideas on specific clinical questions which have not yet been answered, and allied scientists provide the best possible analysis with excavation of the data and extraction of invisible, yet clinically useful information. We approach quickly the destination bearing the name ‘precision medicine’. ■