BACKGROUND AND AIMS
Oestrogen deficiency associated with premature ovarian insufficiency (POI) results in increased osteoclastic activity leading to decreased bone density, earlier onset osteoporosis, and increased fracture risk. Hence, evaluation of baseline bone health is recommended for all women diagnosed with POI, including adolescents. Conventionally, bone health is assessed by a dual-energy X-ray absorptiometry (DEXA) scan, which quantitatively analyses bone mineral density (BMD). However, bone strength depends not only on bone density, but also on bone microarchitecture. Trabecular Bone Score (TBS) evaluates bone microarchitecture by textural analysis of lumbar spine DEXA images, with only a few studies in POI.1-3 Already existing fractures can be detected by Vertebral Fracture Assessment (VFA). The objective of this study was to assess bone health by TBS in women with POI and how it correlates with BMD.
MATERIALS AND METHODS
This was a prospective, cross-sectional study undertaken from April 2024–October 2025 after obtaining ethical approval. The trial was registered under Clinical Trials Registry India (CTRI). Women with POI, meeting all following criteria, were enrolled: age <40 years; primary amenorrhoea or secondary amenorrhoea for at least 4 months; and elevated follicle-stimulating hormone (FSH) >25.0 IU/L on two occasions at least 4 weeks apart. Exclusion criteria included history of surgery on tubes/ovaries, post radiation, post chemotherapy, history of chronic renal disease, untreated thyroid disorders, and corticosteroids/anticonvulsant treatment.
All eligible subjects underwent a DEXA scan to measure BMD, TBS, and VFA. BMD was measured at lumbar spine (L1–L4) and left hip. TBS was measured at lumbar spine (L1–L4) using TBS iNsight™ (Medimaps Group, Geneva, Switzerland) software installed in the DEXA machine. Images at T6–L4 levels were used for VFA.
DEXA scan T-scores of >–1.0, –1.0–-2.5, and <-2.5 indicated normal bone density, osteopenia, and osteoporosis, respectively. TBS scores of >1.35, 1.2–1.35, and <1.2 reflected dense trabeculae with good bone microarchitecture, partially degraded microarchitecture, and degraded microarchitecture with high susceptibility to vertebral fracture, respectively. VFA could detect any wedge, biconcave, or crush fractures.
RESULTS
A total of 50 women with POI were enrolled: seven had primary amenorrhoea and 43 had secondary amenorrhea. Mean age was 25.47 years. Only 11 (22%) had normal bone density, 16 (32%) had osteopenia, and 23 (46%) women were osteoporotic.
Among the 11 women with normal BMD, illustrated by pink in Figure 1, who would be labelled as having good bone health, only 6/11 (54.5%) had good microarchitecture, and the other 5/11 (45.5%) had a TBS of 1.2–1.35. None had a TBS <1.2. In 16 women with osteopenia,, illustrated by purple in Figure 1, three, 11, and two women, respectively, had a TBS <1.2, 1.2–1.35, and >1.35. Thus, 68.7% of women had a TBS of 1.2–1.35, indicating that degradation has started, only 12.5% maintained good architecture and 18% had a TBS <1.2. Among the 23 women who were osteoporotic, illustrated by gray in Figure 1, none had a TBS score of >1.35. Respectively, 18 and five women had a TBS of 1.2–1.35 and <1.2.
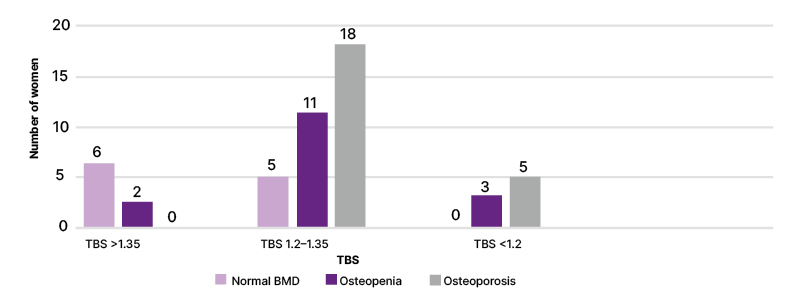
Figure 1: Distribution of women with POI according to TBS and BMD, N=50.
BMD: bone mineral density; POI: primary ovarian insufficiency; TBS: Trabecular Bone Score.
Overall, only 6/50 (12%) women with POI had good bone health, in terms of both BMD and TBS. Figure 1 shows correlation between TBS and BMD. VFA-detected fractures were present in 3/50 (6%) women with POI. Of these three women, one had osteoporosis and two had osteopenia; none had a TBS of >1.35 and two had a TBS of <1.2.
CONCLUSION
TBS is a complimentary tool in the evaluation of bone health, as it assesses bone architecture and compliments fracture risk evaluation by BMD on DEXA scans. The combination of BMD, TBS, and VFA has the potential for early detection of poor bone health in women with POI. Early diagnosis of poor bone health may alleviate long-term consequences through timely counselling, lifestyle modifications, and intervention.






