BACKGROUND AND AIMS
Acute exacerbations of COPD requiring invasive mechanical ventilation represent a severe clinical state associated with high morbidity and mortality.1,2 Despite advances in critical care, contemporary nationwide data describing outcomes in this population remain limited.2 Understanding demographic and clinical factors associated with mortality may improve risk stratification and inform management in critically ill patients with COPD.3 The study aimed to evaluate in-hospital outcomes and identify independent predictors of mortality among adults hospitalized with COPD exacerbations requiring invasive mechanical ventilation using a nationally representative US inpatient cohort.3
MATERIALS AND METHODS
A retrospective analysis of the 2021 National Inpatient Sample (NIS) was performed.4 Adults aged ≥18 years hospitalized with COPD exacerbation (ICD-10 code J44.1) receiving invasive mechanical ventilation (5A19) were included. The primary outcome was in-hospital mortality. Secondary outcomes included length of stay and total hospital charges. Survey-weighted multivariable logistic regression was conducted to identify predictors of mortality. Model calibration was assessed using the Hosmer-Lemeshow test and discrimination with area under the curve.
A total of 76,680 unweighted hospitalizations met inclusion criteria. The mean age was 67±13 years, and 57% of patients were female.3 Overall in-hospital mortality was 28.4%.3 Adjusted predictors of in-hospital mortality identified on multivariable logistic regression analysis are presented in Figure 1. Female sex, Medicaid insurance, private insurance, and self-pay status were associated with lower adjusted odds of mortality, whereas Hispanic race and “Other” race categories demonstrated increased mortality risk. Model calibration demonstrated good fit with a Hosmer-Lemeshow p-value of 0.76, while discrimination analysis yielded an area under the curve of 0.72.3
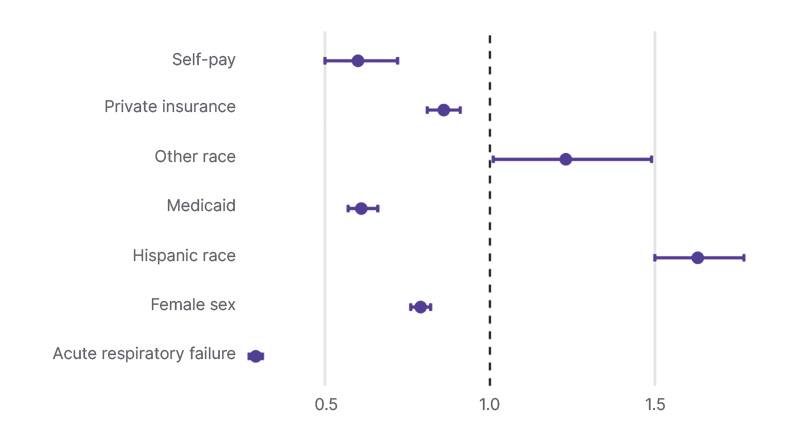
Figure 1: Multivariable-adjusted predictors of in-hospital mortality in mechanically ventilated COPD exacerbations.
Forest plot demonstrating adjusted odds ratios with 95% CIs derived from survey-weighted multivariable logistic regression analysis. Female sex, Medicaid insurance, private insurance, self-pay status, and acute respiratory failure coding were statistically associated with lower odds of in-hospital mortality, whereas Hispanic race and “Other” race categories were associated with increased mortality risk.
RESULTS
Nearly one-third of patients hospitalized with COPD exacerbations requiring invasive mechanical ventilation died during hospitalization, highlighting the severity of illness in this population.2,3 Differences in mortality across race and insurance groups suggest persistent disparities in outcomes that may reflect differences in access to care, comorbidity burden, or treatment patterns. The inverse association observed with acute respiratory failure coding likely reflects heterogeneity in coding practices rather than a true protective effect. Despite advances in ventilatory strategies and critical care management, mortality remains substantial in this population.2,3,5
CONCLUSION
COPD exacerbations requiring invasive mechanical ventilation are associated with high in-hospital mortality.3 Significant variation in outcomes across demographic and socioeconomic groups highlights the need for improved risk stratification and more equitable delivery of care. Standardization of administrative coding and further investigation into drivers of observed disparities are warranted.