
Abstract
Currently, evidence concerning electronic cigarette (e-cigarette) use in the West Indies is unavailable. This study examines the prevalence and associated factors of e-cigarette use in young Trinidadian adults, 6 years after e-cigarettes were introduced in Trinidad. Young adults between the ages of 18 and 40 years were surveyed from May–June 2016. Based on the survey results, descriptive statistics and logistic regression models were used to identify correlations in e-cigarette use. The prevalence of those who had used e-cigarettes was 24.6%, and 41.9% of these people had used both e-cigarettes and tobacco cigarettes. A high proportion (16.95%) of those who had never used tobacco cigarettes had used e-cigarettes. Males were twice as likely as females to have used e-cigarettes (odds ratio [OR]: 2.60; 95% confidence interval [CI]: 1.85–3.68), and participants aged 18–25 years were more likely than those aged 36–40 years to use e-cigarettes (OR: 0.37; 95% CI: 0.14–0.81). The predictors of e-cigarette use as assessed by univariate analysis were current tobacco cigarette smoking (OR: 9.34; 95% CI: 6.14–14.39; p<0.001) and the belief that e-cigarettes are dangerous to health (OR: 0.61; 95% CI: 0.44–0.85; p=0.004). The predictors as assessed by multivariate logistic regression (adjusted OR) were ethnicity (p=0.043), education (p=0.012), and age group (p=0.007). Those who quit using tobacco cigarettes were 7.98 times more likely to use e-cigarettes (95% CI: 4.21–15.45), and those who knew that e-cigarettes contain nicotine were 2.70 times more likely to use them (95% CI: 1.53–4.86; p<0.001). Two summative scales were constructed that measured knowledge and perception. The perception scale, but not the knowledge scale (Cronbach’s alpha=0.736), was a significant predictor of e-cigarette use. The number of e-cigarette users is high (24.6%) in young adults in Trinidad and in those who have never smoked tobacco (16.95%). Current smokers, as well as those who have quit smoking, are at an increased risk of e-cigarette use. This study established that young adults have a low level of knowledge regarding e-cigarettes and shows that they should be educated on e-cigarette use. Further research to examine the reasons for, and susceptibility to, e-cigarette use is necessary.
INTRODUCTION
Electronic cigarettes (e-cigarettes), also known as electronic nicotine delivery systems (ENDS), allow users to inhale an aerosol (vapour) containing flavoured agents, additives, and typically nicotine (though not always), by heating a solution of propylene glycol and/or glycerine. The battery-powered device becomes activated on inhalation, vapourising the liquid to form an aerosol that is then ‘vaped’ into the lungs via a mouthpiece. Vaping provides the same nicotine experience as tobacco cigarettes, while the heated vapour mimics the ‘throat hit’ that occurs in tobacco smoking and is regarded as a vital experience for smokers. These devices are now the most common type of alternative nicotine delivery system used in several countries.1
E-cigarettes are being used increasingly and rapidly among the youth population and young adults.2 Reid et al.3 reported a high use of e-cigarettes in Canadian youth populations and young adults, and McMillen et al.4 found that young adults were at the highest risk of using alternative tobacco products. Traditional media channels that were once used to encourage tobacco cigarette use now use the same aggressive marketing techniques to target young people, advertising e-cigarettes as smoking cessation aids5 that provide a safe, tobacco-free, alternative smoking experience. There is limited evidence regarding the health effects of e-cigarettes. Observational data examining the long-term effects of e-cigarette use are not available and the levels of toxic constituents can vary between products. Though the majority of harmful substances found in tobacco smoke are absent in e-cigarette aerosols, evidence of decreased harm with long-term use is not available6 and short-term e-cigarette use has been associated with adverse events, ranging from a cough, sore throat, shortness of breath, and vomiting, to serious reports of pneumonia, hypotension, and seizures.7 The current research on e-cigarettes is complex and confounded by the wide variation in e-cigarette product composition. Despite being introduced as an aid to smoking cessation, Barrington-Trimis et al.8 have presented data that suggested e-cigarettes may act as gateway agents to the development of a nicotine addiction. Nevertheless, it is estimated that the e-cigarette market, fuelled by the perception of a healthier alternative to smoking, will display a compound annual growth rate of 35% over the period of 2016–2021 and reach a total market size of $10.687 billion by the end of 2021.9 Cognizant of the lack of progress made in decreasing tobacco use in adolescents and young adults, the U.S. Food and Drug Administration (FDA) banned e-cigarette use in minors (<18 years) and began regulating the manufacture, import, packaging, labelling, advertising, promotion, sales, and distribution of ENDS in August 2016.10
When ENDS were first used in the Anglophone Caribbean between 2010 and 2011, they had already been banned in Australia, Brazil, Canada, Israel, Mexico, Panama, and Singapore. The devices were not welcomed by the medical community in Barbados11 and Jamaica.12 In Trinidad and Tobago, e-cigarettes were first introduced in 2010, ironically when the Tobacco Control Act took effect, banning smoking in public places. At present, they remain untouched by regulatory controls. A 2014 report in a popular daily newspaper in the country stated that e-cigarettes were economically attractive, costing $30–90 (1 USA $=6.7 Trinidad Tobago $), and stated: “The bottles of liquids are selling like wildfire.”13 There is no information available on the prevalence and characteristics of e-cigarette users in Caribbean youth and young adults. Therefore, we examined the prevalence and associated factors of ENDS use, knowledge, and perceptions among young adults (18–25 years) in Trinidad. The findings from this study will aid the understanding of the characteristics of young adults who use e-cigarettes and will encourage the development of regulatory controls in Trinidad.
METHODS
This cross-sectional study was undertaken from May–June 2016 by convenience sampling in consenting young adults aged between 18 and 40 years. Participants were recruited from popular locations frequented by young adults across the island, including the Gulf City Mall in the south, Movie Towne at Port-of-Spain in the west, Trincity Mall in the east, and the University campuses of the West Indies and Faculty of Medical Sciences in the north-central part of the island. Validated questionnaires are not available on e-cigarette use. However, the questionnaires we used were pilot-tested using trained interviewers. Data analysis by SPSS version 24 produced descriptive statistics and a logistic regression model was used to identify correlates of e-cigarette use. Pearson’s chi-squared test and the two-sample t-test were used for the univariate analyses, depending on whether the variable being studied was categorical or continuous, respectively. Variables were considered significant if the p-value was <0.05.
The following definitions were used:
- Smoking status was recorded based on self-reporting. A ‘current smoker’ was defined as someone who answered ‘Yes’ to the question: ‘Have you smoked ≥100 cigarettes in your entire life?’ and had smoked a cigarette in the past 28 days.
- A ‘quitter’, or ‘former smoker’, was defined as someone who had smoked >100 cigarettes in their lifetime but had not smoked in the last 28 days.
- A ‘never smoker’ was defined as someone who had not smoked >100 cigarettes in their lifetime and was not a smoker at the time of study.
RESULTS
The dependent variable was binary in nature. The two categories of participants involved were those who had used e-cigarettes and those who had never used e-cigarettes. Table 1 shows the breakdown of the demographic variables and the dependent variable. Of the 911 participants approached, 777 completed the interview (response rate: 85.3%). Non-responders did not participate in the questionnaire largely because of time constraints, and few participants refused to take part. A total of 24.6% (191) of subjects had used an e-cigarette before. Most participants (70.1%) were aged 18–25 years old, 49.9% were of East Indian descent, and the female and male proportions were 50.6% and 49.4%, respectively. The African population was the least represented cohort in the sample (21.2%). The majority of participants (74.9%) had either completed, or were in, current tertiary education. Among the demographic variables, the univariate analyses showed that sex (odds ratio [OR]: 2.60; 95% confidence interval [CI]: 1.85–3.68; p<0.001), and ethnicity (p=0.002) were both significant. In addition, the odds of males having used an e-cigarette before were 2.60 (95% CI: 1.85–3.68) times more likely than females. Subjects aged 36–40 years were significantly less likely (OR: 0.37; 95% CI: 0.14–0.81) to use e-cigarettes compared with those in the 18–25 year age group (p=0.023). Additionally, East Indians (OR: 2.38; 95% CI: 1.48–3.98; p=0.001) and those belonging to other ethnicities (OR: 2.26; 95% CI: 1.34–3.90; p=0.003) were more likely to have tried/used e-cigarettes.
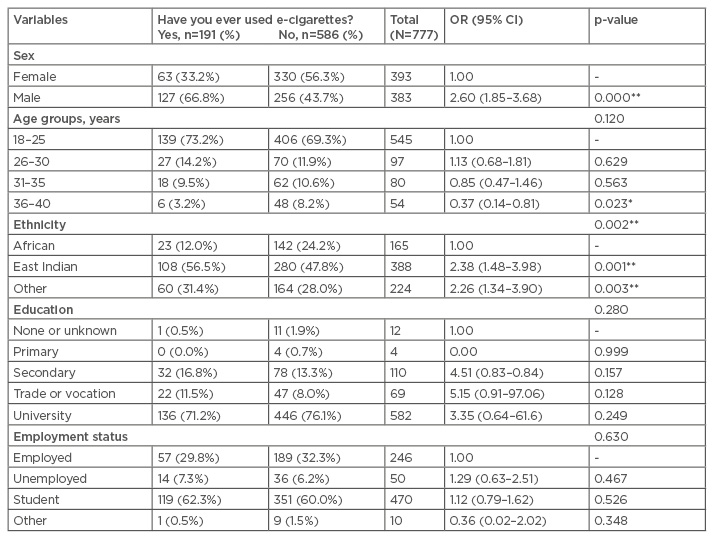
Table 1: Study population profile.
*: p≤0.05; **: p≤0.01.
CI: confidence interval; OR: odds ratio.
Dual use of tobacco cigarettes and e-cigarettes was observed in nearly 42% of subjects. Table 2 shows the univariate analyses among the non-demographic variables that might influence the dependent variable. The variables that were significant predictors of the use of e-cigarettes were binary variables that measured the habit of smoking tobacco, specifically whether someone smoked tobacco cigarettes at the time of study (OR: 9.34; 95% CI: 6.14–14.39; p<0.001), had quit smoking tobacco cigarettes (OR: 8.65; 95% CI: 5.21–14.46; p<0.001), whether the person thought it was dangerous to his/her health (OR: 0.61; 95% CI: 0.44–0.85; p=0.004), and whether they felt that e-cigarettes were safer than tobacco cigarettes (OR: 2.59; 95% CI: 1.86–3.62; p<0.001). Respondents who smoked tobacco cigarettes at the time of study and those who had quit smoking tobacco cigarettes were significantly more likely to have used e-cigarettes in the past. A total of 16.95% of participants who had never smoked a tobacco cigarette previously had used e-cigarettes before.
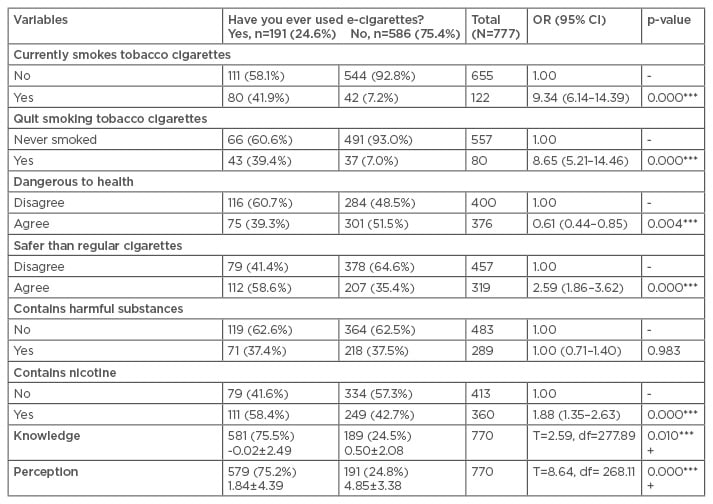
Table 2: Univariate analysis of base characteristics to assess predictors of e-cigarette use (unadjusted odds ratios).
+: p-values result from Welch’s, two-sample independent t-test; *: p≤0.1; **: p≤0.05; ***: p≤0.01.
CI: confidence interval; df: degrees of freedom; OR: odds ratio.
Safety variables also play a role in determining an individual’s predisposition to use/try e-cigarettes. Those who agreed that e-cigarettes were dangerous to health were less likely (OR: 0.61; 95% CI: 0.44–0.85) to have tried/used the devices, while those who agreed that e-cigarettes were safer than regular tobacco cigarettes were more than twice as likely (OR: 2.59; 95% CI: 1.86–3.62) to have used/tried e-cigarettes. Respondents’ knowledge of the toxic content of e-cigarettes was not a significant predictor of e-cigarette use or trial. However, those who knew that e-cigarettes contain nicotine were almost twice as likely to have used an e-cigarette before (OR: 1.88; 95% CI: 1.35–2.63) compared to those who did not.
Two summative scales were constructed that measured knowledge and perception. The summative scale for knowledge consisted of seven questions. The questions included topics such as whether e-cigarettes are cheaper than regular tobacco cigarettes, if e-cigarettes contain nicotine or harmful substances, if users are less likely to develop a habit with e-cigarettes than regular cigarettes, and whether users of e-cigarettes are less likely to develop cancer, heart disease, or lung disease. The summative scale for perception consisted of 10 questions. These included whether e-cigarettes are perceived as dangerous to the health of users, safer than regular tobacco cigarettes, if e-cigarette use is acceptable in public, if e-cigarettes are safe to be used by pregnant women or near children, and if they should be sold to children. Other questions included whether respondents believed regulations should be instigated for e-cigarette use in public, whether a minimum age limit should be enforced for their use, and whether e-cigarettes should be openly advertised.
The reliability of these scales was examined using Cronbach’s alpha.14 A Cronbach’s alpha >0.7 is a good indicator of a reliable scale. The perception scale was more reliable (Cronbach’s alpha: 0.736) than the knowledge scale (Cronbach’s alpha: 0.367). There were statistical differences in the mean knowledge (t=2.59; degrees of freedom: 277.89; p=0.010) and mean perception (t=8.64; degrees of freedom: 268.11; p<0.001) between those who had and those who had never used an e-cigarette.
A multivariable logistic regression with adjusted odds ratio (AOR) (Table 3) identified the variables that were significant predictors, while accounting for the presence of the other variables. The demographic variables of ethnicity (p=0.030), education (p=0.012), and age group (p=0.007) were all significant. In addition, an individual who had quit smoking tobacco cigarettes was almost eight times more likely to use e-cigarettes (OR: 7.98; 95% CI: 4.21–15.45). Those who said e-cigarettes contained nicotine were almost three times more likely to have used them before (OR: 2.70; 95% CI: 1.53–4.86). Out of the perception and knowledge scales, only the perception scale proved to be significant (OR: 0.78; 95% CI: 0.70–0.86; p<0.001). For each unit increase in the perception scale, the odds of trying/using e-cigarettes decreased by 0.78 times.
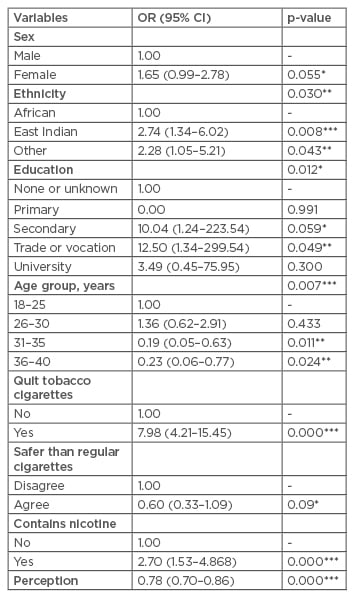
Table 3: Multivariable logistic regression output (adjusted odds ratios).
Results from two-sample independent t-tests.
*: p≤0.1; **: p≤0.05; ***: p≤0.01.
CI: confidence interval; OR: odds ratio.
DISCUSSION
We have explored the pattern of e-cigarette use among young West Indian adults; this was the first such study to our knowledge. ENDS were introduced to Trinidad and Tobago in 2010. Six years later, close to 25% of young adults aged 18–40 years have used an e-cigarette and, of these, 41.9% (n=80) are tobacco cigarette smokers.
Young adults aged 18–25 years and included in this study were more likely to use ENDS. For a country with a population of 1.3 million, this equates to a sizeable proportion of young adults using e-cigarettes, only 6 years after their introduction, and is worrying in the context of international reports. Gravely et al.15 investigated 10 countries with a mix of economic levels in the International Tobacco Control Surveys for self-reported awareness, current usage, and trial of e-cigarettes, and found that e-cigarette use had rapidly increased between 2009 and 2013. In a 2014 CDC National Centre for Health Statistics report, 7 years after ENDS were introduced, 20% of people aged 18–24 years had used an e-cigarette at least once,16 also demonstrating a high progression in e-cigarette use. The number of adults who used ENDS in the European Union (EU) increased from 7.2% to 11.6% during the period of 2012–2014.17 In the UK the number of young people aged 11–18 years who had ever smoked an e-cigarette rose significantly, from 4.6% in 2013, to 8.2% in 2014.18 Adult smokers perceive e-cigarettes as less harmful than tobacco cigarettes, and as an aid to help cut down on or quit smoking, without being trapped by smoke-free policies or emitting second-hand smoke; however, for young people, the market presents e-cigarettes as novel smoking devices with appealing flavours.19
In Trinidad, it is a concern that the prevalence of e-cigarette use has considerably increased in the last 6 years since their introduction, and could rapidly rise to a figure as high as in the UK and the USA. A further concern is that e-cigarettes may become a gateway to smoking in young adults. A longitudinal 2-year study in a cohort of American adolescents and young adults showed that e-cigarette use at baseline progressed to tobacco smoking,20 and, in another report, e-cigarette adolescent users had >6 times the odds of starting cigarette smoking than those who had never used an e-cigarette before.8 More recently, Spindle at al.21 reported that American college students who had used an e-cigarette before were likely to progress to tobacco cigarette smoking after a year, and men were more likely to try these devices. Future research is necessary to monitor the patterns of use in this group to determine whether e-cigarettes provide a trajectory to regular tobacco use. Africans were less likely to try or regularly use ENDS, which may reflect their poorer representation in the study. Further research should explore the sociodemographic differences in e-cigarette use, and the possibility that this habit may be a social/cultural phenomenon favoured by East Indians. Studying the knowledge, beliefs, and health risk perceptions among Trinidad’s multi-ethnic population allows an understanding of e-cigarette use and will inform future practices.
We found that e-cigarette users had higher OR of current tobacco cigarette smoking (OR: 9.34), and quitting (AOR: 7.98) compared to those who had never smoked tobacco cigarettes. Schoenborn and Gindi16 reported that adults from the USA who were current smokers, and former smokers who had quit in the past year, were more likely to use e-cigarettes than people who had never smoked or former smokers with a history of quitting >1 year ago. The International Tobacco Control surveys in Australia and the UK reported e-cigarette use had significantly increased between 2010 and 2012 among current and former smokers in both countries.22 Our findings showed that young adults who had never smoked tobacco cigarettes were not attracted to e-cigarettes or the experience, and this was also observed in research from the USA.16,23 The majority of these study populations were between the ages of 18 and 44 years. In 27 EU countries, among 26,566 youth and adults, 1.2% of those who had never smoked a tobacco cigarette before had used an e-cigarette before, and smokers who had quit in the past year (AOR: 2.08; 95% CI: 1.67–2.58) had a higher likelihood of e-cigarette use.24 This study did not assess how much time had passed since the smokers had quit their tobacco-cigarette smoking habit.
We found that a high proportion, nearly 42%, of e-cigarette smokers were dual users with tobacco cigarettes. High rates of dual use in youth populations has shown that e-cigarettes are not being used as a substitute for tobacco cigarettes.25,26 Future studies are necessary to confirm this finding, since dual users are at high risk of resuming tobacco use.27 E-cigarettes have not been well-studied for harm reduction or as a cessation strategy, and drug regulatory bodies have not approved them as a smoking cessation device. This study did not assess why users of e-cigarettes were deciding to use the devices, and future research should examine the reasons why Trinidadian youth and young adults choose to use e-cigarettes.
The knowledge that e-cigarettes contain nicotine and the perception that e-cigarettes are safer than tobacco cigarettes were predictors of use. It appears that users of e-cigarettes want to have the nicotine experience from the e-cigarette, without the harmful effects associated with tobacco cigarettes. The summative knowledge scale incorporated issues on e-cigarette content, habit forming tendency, and the potential to cause cancer and heart disease. However, knowledge was not a predictor of use; therefore, this gap should be addressed to provide information and encourage awareness in young adults. We believe this finding could be due to contradictory information being readily available as a result of aggressive marketing promotions and vested interests. The perception scale items that were useful in our study delved into the underlying concepts of safety and regulatory controls for pregnant women, children, and advertising. Respondents associated e-cigarette use with harm during pregnancy and to children, and unregulated marketing made respondents less likely to use e-cigarettes. The perception that e-cigarette use is harmful will have implications for public policy and e-cigarette advertising claims.
Our study had some limitations. Being a cross-sectional study, it did not inform on causal relationships between e-cigarette use and independent variables. As all data collected were self-reported, there is the possibility that smoking behaviour was under-reported. The unexpected high rate of refusal to participate at public shopping centres meant data were largely gathered from university students aged 18–30 years, so the results cannot be generalised to all young adults in Trinidad. The study did not assess whether subjects had smoked 100 cigarettes in their lifetime; therefore, we could not use the term ‘former smoker’, rather they were simply called quitters. Furthermore, the study did not explore the reasons for e-cigarette use, and these factors weakened the power of the study. Despite these limitations, the current study does provide an early, valuable insight into the prevalence and correlations of e-cigarette use in young Trinidadian adults. Longitudinal studies to confirm these findings and explore practices of e-cigarette use in this population are recommended.
CONCLUSION
The prevalence of e-cigarette use in young adults in Trinidad has risen rapidly, particularly among those aged 18–25 years, reaching almost 25% 6 years after the introduction of the devices. Current smokers and quitters of tobacco cigarettes are more likely to be e-cigarette users. There are high proportions of dual users of e-cigarettes and tobacco cigarettes, as well as users of e-cigarettes who have never used tobacco cigarettes.






