Abstract
Background: COVID-19 has been declared a global health emergency by the World Health Organisation (WHO). Commonly, a CT chest scan is performed to detect any early findings of COVID-19 pneumonia before the onset of clinical symptoms. In this article, the authors reported COVID-19 pneumonia in patients undergoing positron emission tomography with 2-deoxy-2-(fluorine-18) fluoro-D-glucose integrated with CT (18F-FDG PET/CT) examinations for early isolation and necessary management.
Methods: One hundred and twelve patients who underwent 18F-FDG PET/CT imaging for routine oncological examination were considered for the study, and these subject scans were taken during a period of December 2020–August 2021. Following which, reverse transcription-PCR testing was requested for confirmation.
Results: Amongst the 112 patients, 45 (40%) patients showed features of COVID-19 pneumonia on PET/CT imaging. Reverse transcription-PCR testing carried out for these patients confirmed the infection in 38 individuals (84%).
Conclusion: 18F-FDG PET/CT is sensitive for early detection of COVID-19 pneumonia, so as to minimise further spread of infection and apply adequate measures for prevention.
INTRODUCTION
The novel COVID-19 pneumonia is a continuing global pandemic that has caused deaths of 5 million people worldwide as of November 2021. This aggressive acute respiratory disease occurred in Wuhan, China, in the month of December 2019. After it spread globally, the World Health Organization (WHO) declared COVID-19 a pandemic.1
The majority of individuals present with non-specific symptoms, including a fever, cough, and breathlessness, while others remain asymptomatic. These asymptomatic patients are thought to disperse the infection within the population, and can potentially infect family members.2 Reverse transcription-PCR (RT-PCR) testing remains the gold standard for the diagnosis of COVID-19, even though its sensitivity has been reported as 60–70%.3 No imaging modality has been accepted as the first line of investigation to diagnose COVID-19 pneumonia.4
Ground-glass opacities (GGO) or pulmonary consolidations in multiple lobular and segmental areas are typical findings on chest X-rays and CT scans that are suggestive of COVID-19 pneumonia.5-7 Radiological manifestations of COVID-19 can persist for a while, irrespective of the clinical course.8 As pulmonary parenchymal opacities evolve, progressive atypical respiratory system distress develops, leading to eventual multiorgan failure in few patients.9 It is known that positron emission tomography with 2-deoxy-2-(fluorine-18)fluoro-D-glucose integrated with CT (18F-FDG PET/CT) imaging demonstrates increased uptake in pathologies such as neoplastic aetiologies, inflammatory, and infective processes. Even though 18F-FDG PET/CT imaging is not considered for the primary diagnosis of COVID-19 pneumonia, it is essential to detect infective changes in the chest for further management of patients.10 The incidental use of this type of imaging can detect changes in patients that are asymptomatically infected with COVID-19, and RT-PCR testing can then be used to confirm this diagnosis. It is helpful in terms of patient management on deciding the course of the planned treatment of the underlying disease. It is also important for healthcare workers to undergo necessary safety measures, use personal protective equipment, and sanitise the imaging room at the end of each procedure. Strict containment measures can be undertaken to limit the spread of infection. The rate of asymptomatic infection amongst healthcare workers shows general community transmission; therefore, careful planning is a must to protect staff and patients during an imaging examination.11
The first confirmed case of COVID-19 infection in India was on 27th January 2020. Since then, cases have attained a steady, rising course.12 To suppress this infection, even though there was a nationwide lockdown, hospitals continued to provide comprehensive cancer care with modified protocols and strategies.
The main aim of this study is to highlight occasional radiological findings of COVID-19 pneumonia in patients undergoing 18F-FDG PET/CT examinations and to depict certain considerations to enable a safe scanning process.
MATERIALS AND METHODS
The study was conducted in the authors’ hospital, A. J. Institute of Medical Sciences, Mangalore, Karnataka, India, during a period of eight months from December 2020–August 2021. One hundred and twelve patients who underwent 18F-FDG PET/CT imaging for routine oncological examination on appointment basis were included in the study. Patients considered in this study were asymptomatic at the time of examination and were allowed to undergo the PET/CT study without the need for a negative rapid antigen test or RT-PCR test. However, due to the high prevalence of COVID-19 infection in hospitals, all patients underwent adequate precautions before general access to hospital. According to the hospital’s COVID-19 protocol, patients underwent temperature screening and careful history-taking prior to the initial access to the hospital; based on initial assessment, they were deemed to be asymptomatic for COVID-19 infection. The 18F-FDG PET/CT examination was performed after obtaining informed written consent from patients. The study protocol was approved by the Institutional Research Ethics Committee.
PET-CT Imaging
All the PET/CT images were acquired via the standard protocol using Biograph mCT 20 Time of Flight PET-CT scanner (Siemens Healthineers, Erlangen, Germany), a hybrid 3D PET/CT system. Patients were asked to fast 6–8 hours before the study, and blood glucose levels were kept <200 mg/dL during the time of tracer injection. The scan was performed about 1 hour after an intravenous injection of 0.1 mCi of 18F-FDG/kg, according to the patient’s weight. The acquisition started with non-contrast CT in a cephalocaudal direction. The scan was performed with the patients’ arms placed above the head and normal breathing. The PET data were acquired using a whole body protocol, from vertex to mid-thighs. All emission scans were performed in 3D mode, and the acquisition time per bed position was 2 minutes. Immediately after PET scanning, a contrast-enhanced CT scan was performed using the following parameters: 350 mA, 120 kV, and 5 mm slice thickness. Iodinated non-ionic contrast agent OmnipaqueTM 350 (GE Healthcare, Boston, Massachusetts, USA) was administered intravenously (100 ml) with a flow rate of 5 mL/sec. The lung CT images were reconstructed by filtered back projection into 512×512 pixel images and iterative reconstruction, lung filter with window setting of 1,600 Hounsfield units window width, and 480 Hounsfield units window level. A dedicated workstation was used to view and interpret the CT, PET-CT, and PET images. The images were interpreted by an experienced nuclear medicine specialist and radiologist. The cases that showed indeterminate findings of COVID-19 pneumonia were reported and, for confirmation, RT-PCR testing was requested. The data was then collected, tabulated, and analysed.
RESULTS
Among 112 patients, 64 (57.1%) patients were male and 48 (42.8%) were female. The age group of these patients ranged from 33–78 years, with a mean age of 48.5±3.8 years. Fifty-two patients came for diagnosis and initial PET/CT evaluation; the remaining 60 patients came for follow-up and surveillance scans. Forty patients (35.7%) had lymphoma; 26 patients (23.2%) had lung cancer; 18 patients (16%) had breast cancer; 12 (10.7%) patients had colon cancer; 12 (10.7%) patients had renal cell carcinoma; and four (3%) patients had head or neck malignancies.
Amongst 112 patients, 45 patients (40%) showed high suspicion of COVID-19 pneumonia. These patients were asymptomatic for COVID-19 infection, and lung changes were detected incidentally (Figure 1, 2). Bilateral lung findings were found in 30 patients (66.7%), whereas unilateral lung findings were found in the remaining 15 patients (33.3%). The CT findings included multifocal GGOs and pulmonary consolidations. Pure GGOs were seen in 26 patients (57.7%). Mixed GGOs and pulmonary consolidations were seen in 17 patients (37.7%). One patient had patchy areas of pulmonary consolidation with fibrosis. One more patient had GGO with interlobar septal thickening in bilateral lung fields.
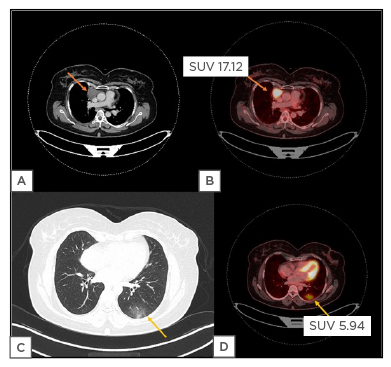
Figure 1: A 47-year-old female patient, with Hodgkin’s lymphoma, was referred for PET/CT evaluation.
Axial contrast enhanced CT image (a) and corresponding fused axial PET/CT image (b) shows a FDG avid anterior mediastinal mass on right side (SUV 17.12). Axial lung window CT image (c) shows unilateral ground-glass opacity in subpleural location of left lower lobe, that shows FDG uptake in corresponding fused PET/CT image (d) with a SUVmax value of 5.94, which was suspicious for COVID-19 pneumonia.
FDG: 2-deoxy-2-(fluorine-18)-fluoro-D-glucose; SUV: standardised uptake value; SUVmax: maximum standardised uptake value.
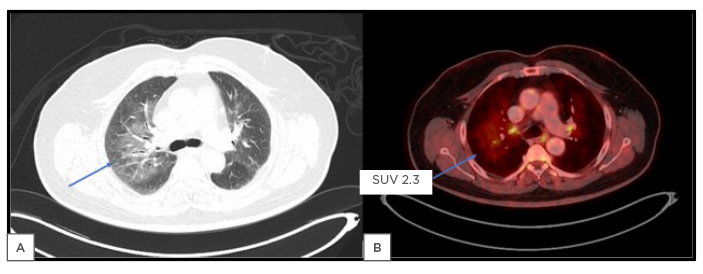
Figure 2: A 70-year-old male patient, another case of Hodgkin’s lymphoma.
Axial lung window CT image (a) shows bilateral ground-glass opacities (right > left) predominantly in perihilar regions, which could suggest infective aetiology. This shows mild FDG uptake in corresponding fused PET/CT image (b) with a SUVmax value of 2.3 (arrows).
FDG: 2-deoxy-2-(fluorine-18)-fluoro-D-glucose; SUV: standardised uptake value; SUVmax: maximum standardised uptake value.
The findings of pneumonia on PET images showed variable FDG avidity. The maximum standardised uptake value (SUVmax) ranged between 1.54–3.0 in 32 patients (71.1%), and between 3.0–7.46 in 13 patients (28.9%). Table 1 shows lung imaging findings and SUVs of the cases considered for the study.
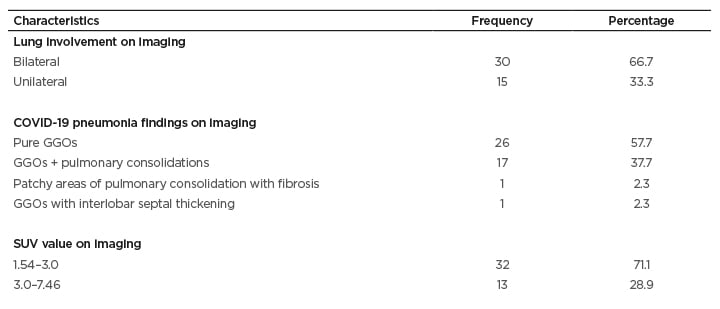
Table 1: Imaging features and demographics of the study population.
GGO: ground glass opacities; SUV: standardised uptake value.
RT-PCR testing was done for these patients within 24–48 hours of imaging, for confirmation of COVID-19 infection. The test was found to be positive in 38 patients (84%). Patients with moderate to severe disease were carefully monitored with the help of medical management and oxygen supplementation, while others were advised for home or institutional quarantine.
DISCUSSION
RT-PCR testing for the diagnosis of COVID-19 has been shown to have lower sensitivity and few studies have shown that positive CT findings with negative RT-PCR result has to be treated as COVID-19 pneumonia.13,14 At present, high-resolution CT imaging of the chest has been chosen as the preferred tool for diagnosis, screening, severity assessment, and monitoring of patients with COVID-19.15,16 CT findings range from pure patchy to multifocal GGOs, to pulmonary consolidations with air bronchograms, which can eventually lead to parenchymal fibrosis. Other ancillary findings include crazy-paving sign, interlobar septal thickening, pleural effusion, reverse halo sign, and reactive lymphadenopathy.17
Since this global pandemic has begun, there have been several case reports, research studies, and investigations in assessing the importance of chest CT in diagnosis, and determining the severity of the disease. Few indices that are used in the clinical practice include the COVID-19 Reporting and Data System (CO-RADS) and CT severity score. However, these indices have been primarily tested in symptomatic patients, and there have not been many studies performed regarding the role of chest CT or other imaging techniques in diagnosis of COVID-19 pneumonia in asymptomatic individuals. A nuclear medicine study, 18F-FDG PET/CT is performed mainly in diagnosis, detection, and staging of malignant lesions.18,19 Apart from malignant tumours, FDG uptake is also seen in active inflammation and infection.20 Since a chest CT component is included in a routine PET/CT study, it would be helpful in diagnosing an asymptomatic cancer patient with COVID-19 pneumonia. Few case reports and studies have been performed in the past showing the presence of COVID-19 pneumonia in patients undergoing FDG PET/CT imaging. It would also be helpful in evaluating the metabolic characteristics of the pulmonary parenchymal opacities, and its FDG uptake.
Few studies and case reports in the past have reported findings of COVID-19 pneumonia in patients who have undergone nuclear medicine imaging studies, including 18F-FDG PET/CT.21,22 In this study of 112 patients, 45 patients (40%) showed COVID-19-associated pneumonic changes in the chest, that were FDG avid on the corresponding PET images (ranged between 1.54–7.46 SUVmax). These results were correlated with the studies performed by Setti et al.,23 Albano et al.,24 and Pallardy et al.,25 who had also incidentally detected COVID-19 pneumonia in patients with cancer who were asymptomatic on 18F-FDG PET/CT examinations. Setti et al.23 detected chest changes in five out of 13 patients whose SUVmax ranged between 4.3–11.3. The study conducted by Albano et al.24 showed typical findings of COVID-19 pneumonia in six out of 65 patients, of which four patients tested positive on RT-PCR testing. Pallardy et al.25 detected abnormalities in 3.8% of patients with cancer who were asymptomatic, with an SUVmax range between 1.58–13.64. One of the authors’ patients had parenchymal consolidation with peripheral GGOs, which is an indeterminate finding of COVID-19 pneumonia (Figure 3). A study conducted by McDermott et al.26 showed that benign GGOs show a significantly higher 18F-FDG uptake in PET/CT than malignant GGOs or nodules, which correlated in this study. These are a few of the studies showing that the risk of spread of infection is increased when patients are referred for routine imaging examinations. Patients who showed incidental lung findings were either undergoing active cancer treatment, or had recently completed treatment. Figure 4 gives a brief summary of the results of this study. The repercussion of cancer disease, as well as cancer treatment, adversely affects the immune system, making patients more susceptible to infection and its complications. Making use of PET/CT in detection of asymptomatic COVID-19 infections in these patients provides an added benefit beyond its oncological aim.27 Few studies also showed the importance of the application of hygienic measures, contact minimisation, and usage of personal protective equipment for the safety and protection of the health personnel as well as patients.28 Another important aspect to be noted is that, once the findings are detected, appropriate action and treatment can be undertaken with clinical monitoring. The main limitation of this study was that the sample size was small; larger studies needs to performed to give accurate results.
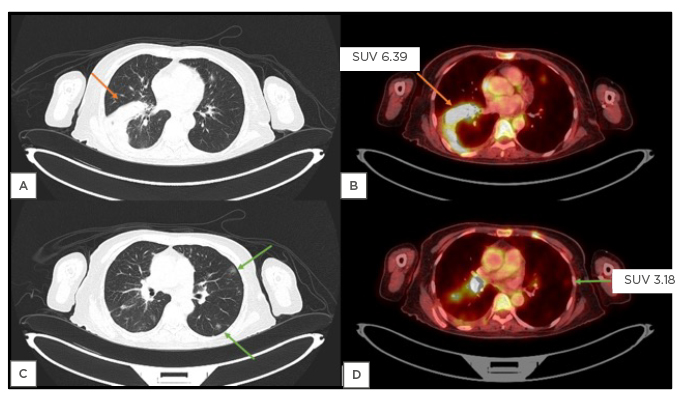
Figure 3: A 58-year-old female patient with of carcinoma of right lateral aspect of tongue.
Axial lung window CT image (a) shows unilateral consolidation in right lower lobe, that shows SUVmax of 6.39 in corresponding fused PET/CT image (b). Axial lung window CT image (c) shows few ill-defined patchy ground-glass opacities in subpleural location of bilateral lung fields (arrows), which shows mild FDG uptake in corresponding fused PET/CT image (d) with a SUVmax value of 3.18. These findings were more in favour of infective aetiology than metastatic disease. Therefore, reverse transcription-PCR test was advised, which was positive.
FDG: 2-deoxy-2-(fluorine-18)-fluoro-D-glucose; SUV: standardised uptake value; SUVmax: maximum standardised uptake value.
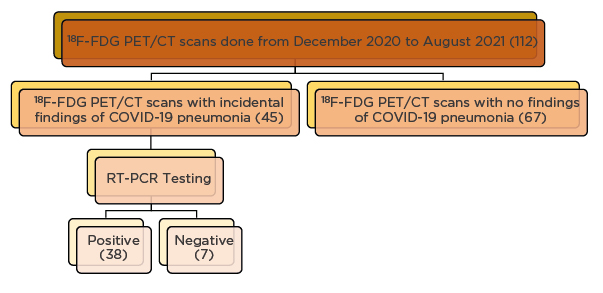
Figure 4: Flowchart depicting the study results and interpretation.
18F-FDG PET/CT: 2-deoxy-2-(fluorine-18)-fluoro-D-glucose integrated with CT; RT-PCR: reverse transcription-PCR.
CONCLUSION
The authors concluded that COVID-19 pneumonia showed SUV uptake on FDG PET/CT imaging and can be detected as an incidental finding in asymptomatic patients. Although FDG PET/CT imaging is not the first-line imaging modality in detecting COVID-19 pneumonia, it can be effectively used during this pandemic. It is advised to undergo adequate safety measures before undergoing any imaging procedure, as well as ensuring the safety of healthcare workers, and the appropriate preparation of imaging services. These measures could not only help in patient management but could also reduce the community spread of infection.