Meeting Summary
Severe asthma is a significant cause of morbidity and mortality estimated to affect 3.7% of patients with asthma. Most patients with severe asthma have Type 2 inflammation, which can be difficult to control despite standard of care with high-dose inhaled corticosteroids (ICS). Add-on biologic therapy is recommended in these patients, and among the currently approved options, depemokimab represents the first ultra-long-acting biologic. Depemokimab efficacy and tolerability over 52 weeks were demonstrated in the Phase III SWIFT-1/-2 studies, and patients who completed these studies were invited to join the subsequent AGILE open-label extension (OLE) study.
This article summarizes data presented at the American Thoracic Society (ATS) 2026 Conference from an integrated analysis of the SWIFT-1/-2 and AGILE OLE studies, reporting long-term efficacy and safety findings from up to 2 years of depemokimab exposure in patients with Type 2 asthma. In addition to overall efficacy and safety, posters included data from subsets of patients receiving medium- and high-dose ICS at baseline, and patients with comorbid chronic rhinosinusitis with nasal polyps (CRSwNP).
These new data provide descriptive insights into the durable, long-term efficacy and tolerability of depemokimab in patients with severe asthma, for up to 2 years, and may provide additional context for clinicians in evaluating biologic treatment options for their patients.
Introduction
Despite advances in asthma management, severe asthma remains a significant cause of global morbidity and mortality.1 Estimated to affect 3.7% of patients with asthma, severe asthma is defined as uncontrolled disease despite adherence to treatment with high-dose ICS and a long-acting β2 agonist.2,3
Most patients with severe asthma have Type 2 inflammation, characterized by the production of cytokines such as IL-4, IL-5, and IL-13; eosinophilia; and increased fractional exhaled nitric oxide.2 Type 2 inflammation can be difficult to control with high-dose ICS, and while it may respond to oral corticosteroids, these are associated with serious side effects.2 Approved Type 2-targeted biologics are therefore recommended as add-on therapy in patients with severe asthma who have eosinophilic or allergic biomarkers, or who require maintenance with oral corticosteroids.2
A total of seven biologics are currently available for severe asthma, including omalizumab, mepolizumab, reslizumab, benralizumab, dupilumab, tezepelumab, and depemokimab.3,4 Among these, depemokimab is the only ultra-long-acting option, with enhanced IL-5 binding affinity, high potency, and extended half-life, enabling twice-yearly dosing in asthma.4-6 Depemokimab is approved for add-on maintenance of severe asthma treatment characterized by an eosinophilic phenotype in adult and pediatric patients aged 12 years and older in the USA.4 It is not indicated for the relief of acute bronchospasm or status asthmaticus.4 Depemokimab is also approved for use in severe eosinophilic asthma in the UK, EU, China, and Japan,7-9 and in CRSwNP in the UK, EU, and China.7-9
The Phase III SWIFT-1/-2 studies demonstrated the efficacy and safety of depemokimab in patients aged ≥12 years with eosinophilic Type 2 asthma over 52 weeks (Figure 1).11 Eligible patients were randomized 2:1 to receive subcutaneous depemokimab 100 mg (n=502) or placebo (n=260) every 26 weeks for 1 year.11
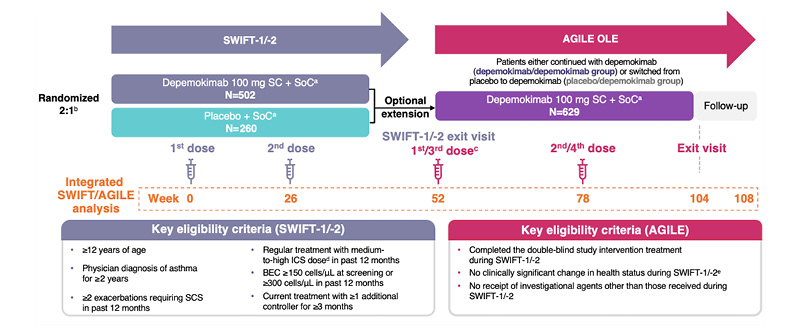
Figure 1: SWIFT-1/-2 and AGILE OLE clinical studies.10
aIncluding treatment with medium-to-high ICS dose plus ≥1 additional controller and excluding biologics.
bDepemokimab:placebo.
cAGILE Visit 1 (SWIFT-1/-2, Week 52) was considered as baseline for AGILE. The exit visit in SWIFT-1/-2 was used as baseline for AGILE if it was on the same day or within 7 days of AGILE Visit 1; however, if Visit 1 was >7 days (max 14 days) after the exit visit, baseline assessments were performed pre-dose at Visit 1.
dDefinitions based on GINA 2021 guidelines.
ePatients excluded only if an investigator deemed that their change in health status made them unsuitable
for participation.
The sample size was determined by the number of available participants who were randomized into SWIFT-1 and SWIFT-2 and who were eligible for the current study based on inclusion and exclusion criteria.
BEC: blood eosinophil count; GINA: Global Initiative for Asthma; ICS: inhaled corticosteroid; OLE: open-label extension; SC: subcutaneous; SCS: systemic corticosteroid(s); SoC: standard of care.
In a pooled analysis of SWIFT-1 and SWIFT-2, depemokimab reduced exacerbations by 54% over 52 weeks versus placebo, along with sustained suppression of inflammation, as assessed by blood eosinophil count (82% reduction in SWIFT-1 and 83% reduction in SWIFT-2 at Week 52).11 Depemokimab also showed numerical improvements versus placebo in patient-reported outcome measures. The change in St George’s Respiratory Questionnaire (SGRQ) total score (standard error [SE]) from baseline to Week 52 with depemokimab versus placebo was −13.92 (0.76) versus −11.04 (1.06), respectively,and in Asthma Control Questionnaire-5 (ACQ-5) score (SE) it was −0.81 (0.05) versus −0.73 (0.06), respectively.11 In prespecified subgroup analyses, depemokimab was found to reduce exacerbations compared with placebo across both medium- and high-dose ICS patient subgroups,12 and in patients with comorbid CRSwNP.13
The overall incidence of adverse events (AE) was similar between depemokimab and placebo treatment groups.11 The most common AEs were upper respiratory tract infection, allergic rhinitis, influenza, arthralgia, and pharyngitis.11 Among patients receiving depemokimab, 72% in SWIFT-1 and 73% in SWIFT-2 had an AE, of which 3% and 4%, respectively, were related to depemokimab and 1% in each study led to discontinuation or withdrawal. A serious AE (SAE) was reported in 6% and 8% of patients, respectively, none of which were considered related to depemokimab. Among patients receiving placebo, 73% in SWIFT-1 and 78% in SWIFT-2 had an AE: 4% and 1%, respectively, were related to placebo, and 2% and 1% led to discontinuation or withdrawal. An SAE was reported in 17% and 10% of patients, respectively.11
The long-term safety and efficacy of depemokimab in asthma was subsequently assessed in the single-arm, 52-week AGILE OLE study (Figure 1).14 Patients who completed SWIFT-1/-2 were invited to join the OLE study. Of the 762 randomized patients, 641 (84%) entered the OLE; 419 continued with depemokimab (depemokimab/depemokimab) and 210 switched from placebo to depemokimab (placebo/depemokimab), with a total follow-up period of 104 weeks. Twice-yearly depemokimab was generally well tolerated up to 104 weeks; AEs occurred in similar proportions of patients in each group (depemokimab/depemokimab: 72%; placebo/depemokimab: 70%), and no treatment-related SAEs were reported. Efficacy was sustained in patients previously treated with depemokimab, and those switching from placebo experienced numerical reductions in exacerbations; annualized exacerbation rates (AER; 95% CI) were 0.55 (0.47–0.66) and 0.58 (0.45–0.73), respectively.14
At the ATS 2026 Conference, data were presented from an integrated post-hoc analysis of the SWIFT-1/-2 and AGILE studies (N=629), reporting long-term data for depemokimab in terms of overall safety and efficacy, efficacy by baseline ICS dose, and efficacy in patients with comorbid CRSwNP.10,15 These data are summarized in this article.
Sustained Long-Term Efficacy and Consistent Patient-Reported Outcomes Over 2 Years in Patients with Type 2 Asthma
In the integrated analysis of SWIFT-1/-2 and AGILE, key patient demographics and baseline characteristics were evenly distributed across treatment groups. Reduction in AER was sustained over the full 2-year SWIFT/AGILE period in the depemokimab/depemokimab group (AER: 0.52 [95% CI: 0.45–0.60]), while those in the placebo/depemokimab group experienced greater reductions in exacerbations versus Year 1 (Figure 2). In addition, time to first exacerbation was longer for patients in the depemokimab/depemokimab group across the 2-year period compared with the placebo/depemokimab group. This difference was less pronounced, however, after Week 52, when all patients received depemokimab.10
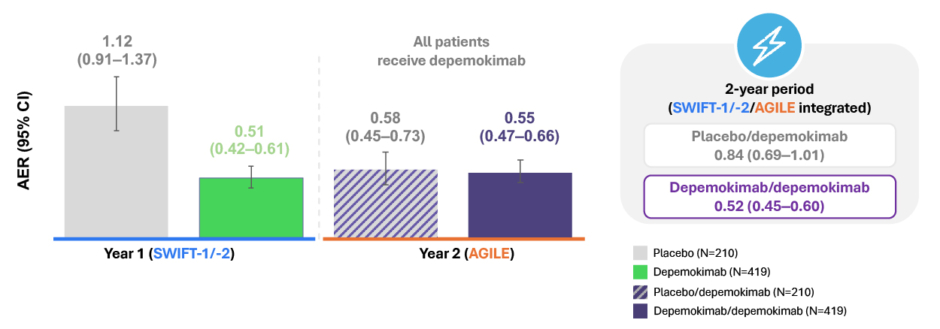
Figure 2: Reduction in AER during the SWIFT-1/-2 and AGILE studies.10,a
aAt pre-SWIFT-1/-2 baseline, the mean (SD) number of exacerbations requiring OCS/SCS in the past 12 months was 2.5 (1.7) in the depemokimab/depemokimab group, and 2.4 (1.1) in the placebo/depemokimab group.
AER: annualized exacerbation rates; OCS: oral corticosteroids; SCS: systemic corticosteroids.
Reductions in SGRQ total score andACQ-5 score were sustained over the 2-year SWIFT/AGILE period in the depemokimab/depemokimab group, and numerical improvements were observed in the placebo/depemokimab group following depemokimab initiation in AGILE. Change from baseline in SGRQ total score (SE) in the depemokimab/depemokimab group was −13.92 (0.76) at Week 52 and −16.29 (0.85) at Week 104. Similarly, change from baseline in ACQ-5 score (SE) in the depemokimab/depemokimab group was −0.81 (0.05) at Week 52 and −0.89 (0.05) at Week 104.10
Eosinophil levels remained suppressed in the depemokimab/depemokimab group over the 2-year period, while those in the placebo/depemokimab group experienced an 85% reduction from baseline in blood eosinophil count following depemokimab initiation. Accordingly, suppression of Type 2 inflammation, as assessed by blood eosinophil count, was consistent throughout the 2-year period in the depemokimab/depemokimab group; the ratio to baseline (SE logs) at Week 104 was 0.174 (0.04).10
Overall, the integrated post-hoc analysis of SWIFT-1/-2 and AGILE showed sustained suppression of inflammation and efficacy over a 2-year period, supporting the long-term efficacy of twice-yearly depemokimab in patients with Type 2 asthma.10
Long-Term Efficacy and Patient-Reported Outcomes by Baseline ICS
In SWIFT-1/-2 (N=762), AER (95% CI) over 52 weeks in the depemokimab group was 0.36 (0.27–0.48) in the medium-dose ICS subgroup and 0.65 (0.53–0.79) in the high-dose ICS subgroup.12 Improvements in SGRQ and ACQ-5 scores were also observed with depemokimab regardless of baseline ICS dose: least squares mean (SE) change from baseline through Week 52 in the medium- and high-dose ICS subgroups, respectively, was −14.38 (1.19) and −13.60 (1.01) for SGRQ, and −0.89 (0.07) and −0.76 (0.06) for ACQ-5.16
In the integrated analysis of SWIFT-1/-2 and AGILE, a similar proportion of patients received medium-dose and high-dose ICS at baseline. Patients receiving high-dose ICS had a history of more exacerbations, higher baseline symptom scores, and higher baseline blood eosinophil counts compared with patients receiving medium-dose ICS.16
Patients in both ICS-dose subgroups experienced reductions in exacerbations with depemokimab versus placebo during SWIFT-1/-2, and these reductions were maintained during the AGILE OLE. In addition, those patients who switched from placebo during SWIFT-1/-2 to depemokimab during AGILE showed reductions in exacerbations following the switch, regardless of baseline ICS dose.16
Among patients in the depemokimab/depemokimab group who received depemokimab throughout the 2-year study period (n=419), 172 patients were on medium-dose ICS at baseline, and 247 were on high-dose ICS. In these patients, AER was maintained over 2 years in both the medium-dose (0.41 [95% CI: 0.32–0.52]) and high-dose (0.62 [95% CI: 0.52–0.75]) ICS subgroups.16
Improvements in SGRQ total score and ACQ-5 score from baseline through Week 52 were also maintained throughout Week 104 in patients receiving medium-dose or high-dose ICS.16
Overall, twice-yearly depemokimab showed sustained efficacy over 2 years, irrespective of baseline ICS dose.16
Long-Term Efficacy and Patient-Reported Outcomes in Patients with Comorbid CRSwNP
Several comorbidities are common in patients with severe asthma, and these can contribute to symptom burden and impair quality of life.2 CRSwNP is a common comorbidity among patients with Type 2 asthma, and is characterized by persistent symptoms such as nasal obstruction, rhinorrhea, facial pain, and loss of smell.17 The presence of CRSwNP is considered a potential predictor of an enhanced response to IL-5 therapy.2
A prespecified analysis of SWIFT-1/-2 (N=762) investigated the efficacy of depemokimab in a subgroup of patients with comorbid CRSwNP (n=113; depemokimab: n=80; placebo: n=33). Overall, there was a 69% (95% CI: 42–83) reduction in AER versus placebo in the CRSwNP subgroup (0.51; n=80 versus 1.61; n=33, respectively) compared with a 51% (95% CI: 36–62) reduction in those without CRSwNP (0.51; n=421 versus 1.03; n=227). SGRQ and ACQ-5 scores also showed greater improvements in the CRSwNP subgroup than in the overall population receiving depemokimab.13
Among 419 patients treated with depemokimab over the full 2 years of the SWIFT/AGILE study period, 66 (15.8%) had comorbid CRSwNP at baseline. Improvements observed in SWIFT-1/-2 were maintained in AGILE, regardless of CRSwNP status; AER (95% CI) was 0.45 (0.31–0.65) for patients with CRSwNP and 0.54 (0.46–0.63) for patients without CRSwNP over 2 years.15
Numerically greater improvements in SGRQ and ACQ-5 scores were also maintained over the 2-year period, regardless of CRSwNP status at baseline, with more pronounced improvements observed in those with CRSwNP.15
Overall, depemokimab showed sustained efficacy over the SWIFT/AGILE 2-year period in patients with Type 2 asthma, regardless of CRSwNP comorbidity status at baseline.15 Comorbid CRSwNP in asthma is indicative that disease is primarily driven by Type 2 inflammation,17 which may explain the enhanced clinical benefit observed with depemokimab in patients with this comorbidity.
Twice-Yearly Depemokimab is Well Tolerated Over 2 Years in Patients with Type 2 Asthma
During the 52-week AGILE OLE, where all patients received depemokimab (N=629), AEs and SAEs were reported in similar proportions of patients across depemokimab/depemokimab and placebo/depemokimab groups. There were no treatment-related SAEs or fatal SAEs, and low rates of adverse events of special interest (AESI).18
The long-term safety of depemokimab over 2 years was assessed in the integrated post-hoc analysis, including AEs, serious AEs, and AESIs reported in patients who received depemokimab for the full 2-year period (n=419; Figure 3).18
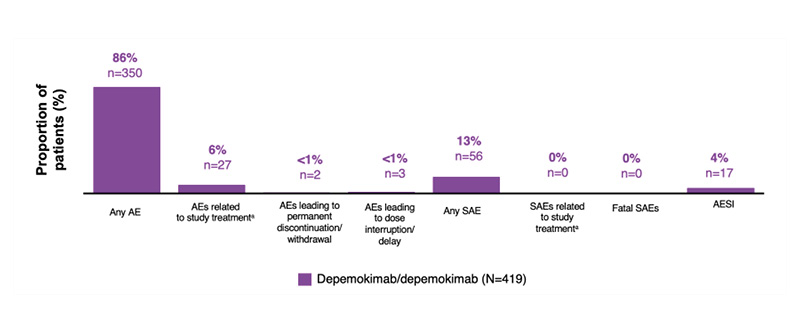
Figure 3: Overview of safety during the SWIFT-1/-2 and AGILE studies.18
ᵃAE/SAE relation to study treatment was assessed by investigator.
AE: adverse event; AESI: adverse event of special interest; SAE: serious adverse event.
AEs were reported in 86% of patients, of which COVID-19 (25%), nasopharyngitis (23%), and upper respiratory tract infection (16%) were the most common. Treatment-related AEs (per investigator assessment) occurred in 6% of patients, of which headache (1%), injection-site reaction (<1%), and leukopenia (<1%) were the most common. AEs leading to discontinuation or dose interruption were infrequent (both <1%), and SAEs occurred in 13% of patients. Asthma (3%) was the only SAE to occur in ≥1% of patients. No treatment-related SAEs (per investigator assessment) or fatal SAEs occurred during the 2-year period.18
AESIs were reported in 4% of patients: nervous system disorders in 2% of patients, general disorders and administration site conditions in 1%, and skin and subcutaneous tissue disorders in <1%. No single AESI occurred in ≥1% of patients. Anti-drug antibodies (ADA) and neutralizing antibodies occurred infrequently, and there was no association found between ADA status and depemokimab efficacy or safety.18
Overall, twice-yearly depemokimab had low discontinuation rates, no treatment-related or fatal SAEs and AESIs, and few ADAs and neutralizing antibodies over the 2-year SWIFT/AGILE period. The most commonly reported AEs were transient in duration and were similar to findings in Phase III programs for asthma and CRSwNP.19
In addition, no significant safety concerns were identified among patients who switched from placebo to depemokimab during the AGILE OLE; the incidence of AEs was similar between treatment groups and when compared with the placebo group in SWIFT-1/-2.11
Conclusion
The integrated analysis of SWIFT-1/-2 and AGILE supports the long-term efficacy and tolerability of twice-yearly depemokimab in patients with Type 2 asthma. The post-hoc analyses showed sustained reductions in AER and maintenance of patient-reported outcome improvements over 2 years of depemokimab treatment.10 Suppression of Type 2 inflammation, assessed by blood eosinophil levels, was also maintained. Findings were similar regardless of baseline ICS dose and comorbid CRSwNP status, with greater reductions in exacerbation rates in patients with comorbid CRSwNP.12,15,16
The safety profile of depemokimab was similar to placebo in Year 1 and remained consistent through Year 2, with no treatment-related or fatal SAEs reported and no new safety concerns identified with long-term depemokimab exposure. Most on-treatment AEs reflected expected events such as COVID-19, nasopharyngitis, and upper respiratory tract infection.18
Overall, these findings provide further insights into the efficacy and safety of twice-yearly depemokimab in patients with severe Type 2 asthma, and durable,long-term effects up to 2 years. The full details of the integrated analysis are expected to be published later this year.
Job code: PSE-US-5218






