BACKGROUND AND AIMS
Primary cardiac involvement (pCI) is a major contributor to morbidity and mortality in systemic sclerosis (SSc). In routine practice, early cardiac manifestations may be under-recognised, particularly when systematic screening is not performed.
This study aimed to determine the baseline prevalence and clinical correlates of pCI in the SOLAR (Systemic Sclerosis Longitudinal Assessment Registry) and to summarise incident pCI during follow-up.1
MATERIALS AND METHODS
The authors conducted a cross-sectional baseline analysis with a longitudinal follow-up description using data from the SOLAR. The baseline cohort comprised 372 patients who fulfilled the 2013 American College of Rheumatology/European Alliance of Associations for Rheumatology (ACR/EULAR) classification criteria for SSc,2 representing an early SSc population with a disease duration of up to 3 years. pCI was defined as myocardial, pericardial, coronary, or conduction system abnormalities attributable to SSc. Baseline demographic, clinical, and laboratory variables were compared between patients with and without pCI using Fisher’s exact test or Welch’s t-test, as appropriate. Follow-up was assessed using available follow-up visits conducted at 6-month intervals to identify incident pCI among patients who were pCI-negative.
RESULTS
At baseline, pCI was present in 24/372 patients (6.5%), and most patients who were pCI-positive were female (79.2%). In available component fields, coronary artery disease was the most frequently recorded manifestation (16/24), whereas heart failure (1/24) and pericardial effusion (1/24) were uncommon. Patients with pCI were older than those without (56.7±15.4 versus [vs] 50.4±12.8 years; p=0.063). Skin subtype distribution differed (p=0.018), with diffuse cutaneous and sine scleroderma proportionally more frequent among patients who were pCI-positive. Myositis (12.5% vs 1.7%; p=0.016), pulmonary arterial hypertension (33.3% vs 3.2%; p<0.001), overlap syndrome (33.3% vs 9.8%; p=0.003), and hypertension (41.7% vs 16.1%; p=0.004) were also more common in the pCI group, while interstitial lung disease showed a non-significant numerical increase (52.2% vs 34.1%; p=0.112). Capillaroscopy patterns were available in 276 patients and were similar between groups (p=0.195), although late patterns were numerically more frequent with pCI (21.1% vs 8.6%; Table 1). Diabetes was numerically higher in the pCI group (16.7% vs 8.3%) but did not reach statistical significance (p=0.252).
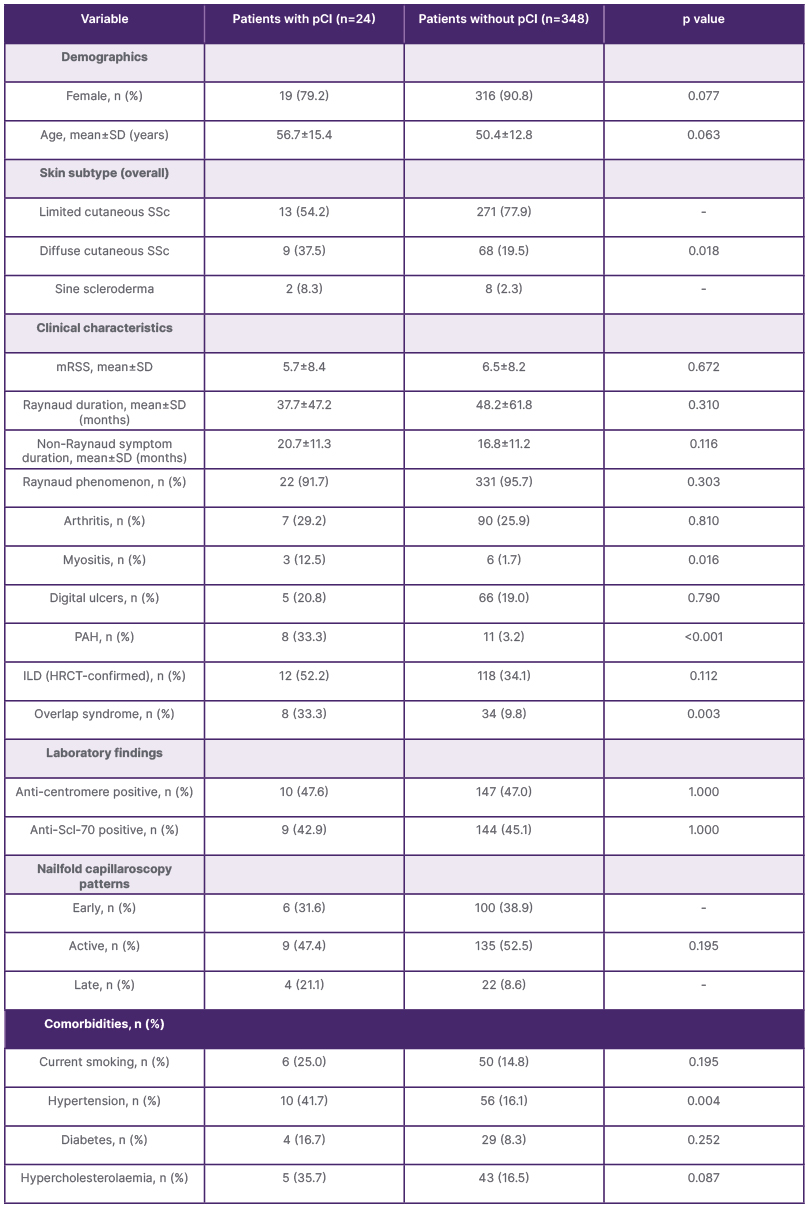
Table 1: Baseline characteristics of patients with and without pCI.
Anti-Scl-70: anti-topoisomerase I antibody; HRCT: high-resolution CT; ILD: interstitial lung disease; mRSS: modified Rodnan skin score; PAH: pulmonary arterial hypertension; pCI: primary cardiac involvement; SSc: systemic sclerosis.
Associated factors for pCI included older age (odds ratio [OR]: 1.04 per year; 95% CI: 1.00–1.07; p=0.024), diffuse cutaneous subtype (OR: 2.47; 95% CI: 1.04–5.88; p=0.041), myositis (OR: 8.07; 95% CI: 1.89–34.56; p=0.005), pulmonary arterial hypertension (OR: 15.27; 95% CI: 5.40–43.20; p<0.001), overlap syndrome (OR: 4.62; 95% CI: 1.84–11.58; p=0.001), and hypertension (OR: 3.72; 95% CI: 1.58–8.81; p=0.003). Limited cutaneous SSc was associated with a lower risk of pCI (OR: 0.34; 95% CI: 0.14–0.78; p=0.011). Among patients without pCI at baseline and with follow-up pCI data (n=275), six (2.2%) developed incident pCI, first detected at visit two in five patients and at visit three in one; overall, 30/372 patients (8.1%) had pCI recorded at least once across visits one to four.
CONCLUSION
In this early SSc registry cohort, pCI was documented in a minority of patients at baseline, which may partly reflect real-world reporting practices and the likelihood that subclinical disease is under-captured in a registry setting. Nevertheless, pCI clustered with a higher-risk clinical profile, particularly diffuse skin involvement, pulmonary arterial hypertension, myositis/overlap features, and hypertension. The emergence of new pCI cases during follow-up suggests that a single baseline assessment may miss evolving cardiac involvement, supporting structured and repeated cardiac evaluation in SSc, especially in patients with multisystem disease.






