Meeting Summary
Androgen deprivation therapy (ADT) has long been the cornerstone of treatment for advanced prostate cancer. Since the introduction of gonadotropin-releasing hormone (GnRH) agonists, the treatment landscape has evolved considerably, with the subsequent development of long-acting injectable and, more recently, oral GnRH antagonists offering clinicians a broader range of therapeutic options. A critical differentiator of these treatments lies in their mechanism of action: while GnRH agonists initially stimulate the hypothalamic-pituitary axis, causing a transient testosterone surge before suppression is achieved, GnRH antagonists competitively block GnRH receptors to achieve rapid, sustained testosterone suppression without the initial flare. The more recent emergence of an oral GnRH antagonist represents a significant step forward, providing a non-injectable ADT option that allows clinicians to tailor treatment based on clinical factors, such as disease burden, comorbidities, and patient preference.
Introduction
At the Accord Healthcare-sponsored symposium (Accord Healthcare Ltd, London, UK), ‘Who, What, When – Clinical Viewpoints on ADT Choice in Prostate Cancer’, held on 14th March 2026 at the European Association of Urology (EAU) 2026 Congress in London, UK, specialists from the UK, Spain, Italy, and the USA shared insights on the increasingly important topic of how to individualise ADT selection in prostate cancer. The symposium aimed to explore expert perspectives on the clinical decision-making process for selecting ADT in prostate cancer, and to enhance understanding of individualised treatment approaches based on patient characteristics and disease profiles.
Oral ADT: Are We Entering a New Era in Treatment?
Alberto Briganti, San Raffaele Hospital, Milan, Italy, opened his session by emphasising that ADT remains the cornerstone of treatment for metastatic hormone-sensitive prostate cancer, used in up to 40% of men with prostate cancer at some point during their treatment journey.1 He provided an overview of the mechanistic differences between GnRH antagonists versus GnRH agonists, highlighting the key physiological distinction: GnRH agonists cause an initial testosterone surge prior to suppression, necessitating short-term antiandrogen co-administration to mitigate testosterone flare. Conversely, GnRH antagonists competitively block GnRH receptors and achieve rapid testosterone suppression without an initial surge.2 Briganti identified three key areas in which GnRH antagonists offer potential clinical advantages over GnRH agonists: cardiovascular (CV) risk reduction, lower urinary tract symptom (LUTS) control, and testosterone suppression and recovery.
Cardiovascular Risk in Patients Initiating ADT
Prostate cancer and cardiovascular disease (CVD) frequently coexist, with data from national cancer registries, such as the Surveillance, Epidemiology, and End Results (SEER) programme, indicating an increased risk of death from heart disease among patients with prostate cancer.3 ADT may contribute to this risk through androgen deprivation-related metabolic disturbances, including altered body composition, dyslipidaemia, impaired glycaemic control, and promotion of atherosclerosis.4
Evidence from a systematic review of RCTs evaluating GnRH antagonists versus agonists in men with prostate cancer demonstrated that antagonists are associated with lower major adverse cardiovascular event (MACE) risk compared with agonists.5 In the HERO trial, a Phase III RCT comparing the oral GnRH antagonist relugolix with the GnRH agonist leuprolide, analysis of the safety endpoints showed that the cumulative incidence of MACE at Week 48 was 2.9% with relugolix versus 6.2% with leuprolide in all patients, and, in a post-hoc analysis, 3.6% versus 17.8%, respectively, in those with a prior history of MACE. The hazard ratio for MACE with relugolix versus leuprolide was 0.46 (95% CI: 0.24–0.88; Figure 1).6
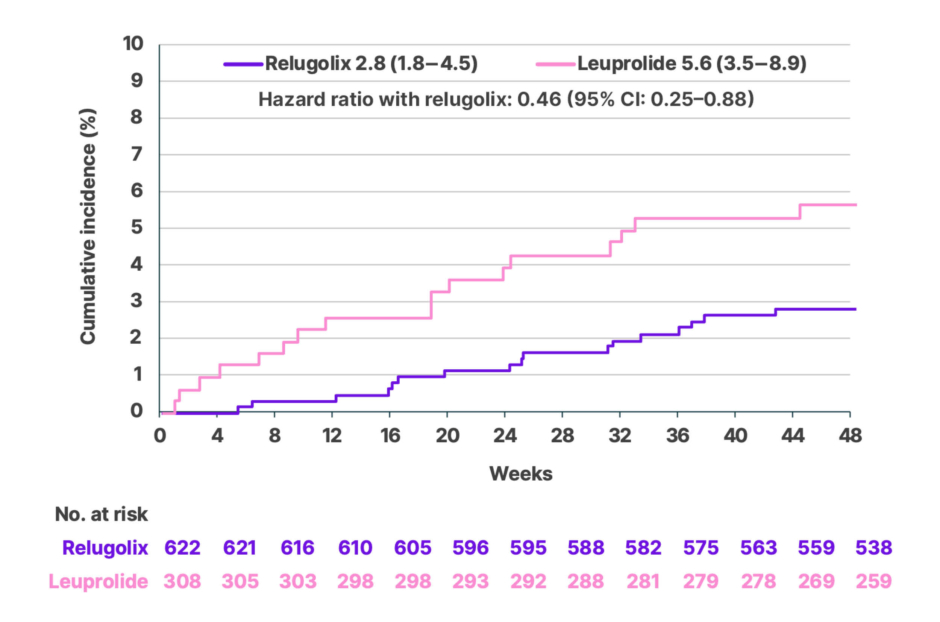
Figure 1: Cumulative incidence of MACE at the end of Week 48 in the HERO trial.6
Adapted from Shore N et al.6
MACE: major adverse cardiovascular event.
Briganti also referenced the 2022 European Society of Cardiology (ESC) Cardio-Oncology Guidelines, which recommend baseline CV risk assessment and annual monitoring during ADT, and which advise that a GnRH antagonist should be considered in patients with pre-existing symptomatic coronary artery disease who require ADT.7 The EAU 2024 Guidelines similarly acknowledge that CV side effects may be less frequent with GnRH antagonists, and recommend their consideration in patients with pre-existing CVD or multiple CV risk factors.8
Lower Urinary Tract Symptoms
Briganti noted that moderate-to-severe LUTS are common in men with prostate cancer, referencing a prospective single-centre study where over 44% of cases with newly diagnosed localised prostate cancer were found to have moderate-to-severe LUTS at baseline.9
Briganti presented data from a pooled analysis of three Phase III RCTs of once-monthly treatment for 12 weeks with GnRH antagonist degarelix (240/80 mg; n=289) or GnRH agonist goserelin plus bicalutamide (50 mg; n=174). Patients receiving degarelix compared with the GnRH agonist had significantly greater decreases in IPSS versus GnRH agonist at Week 12 (adjusted difference: −1.24; 95% CI: −2.33–−0.14; p=0.03). Clinically relevant LUTS relief with degarelix was especially pronounced in patients with moderate-to-severe LUTS (baseline IPSS ≥13; odds ratio: 2.31; 95% CI: 1.19–4.47; p=0.01) and advanced prostate cancer (odds ratio: 2.36; 95% CI: 1.10–5.04; p=0.03; Figure 2).10 These results suggest a clinically meaningful benefit of GnRH antagonist therapy in patients with prostate cancer and moderate-to-severe LUTS (IPSS ≥13).10,11
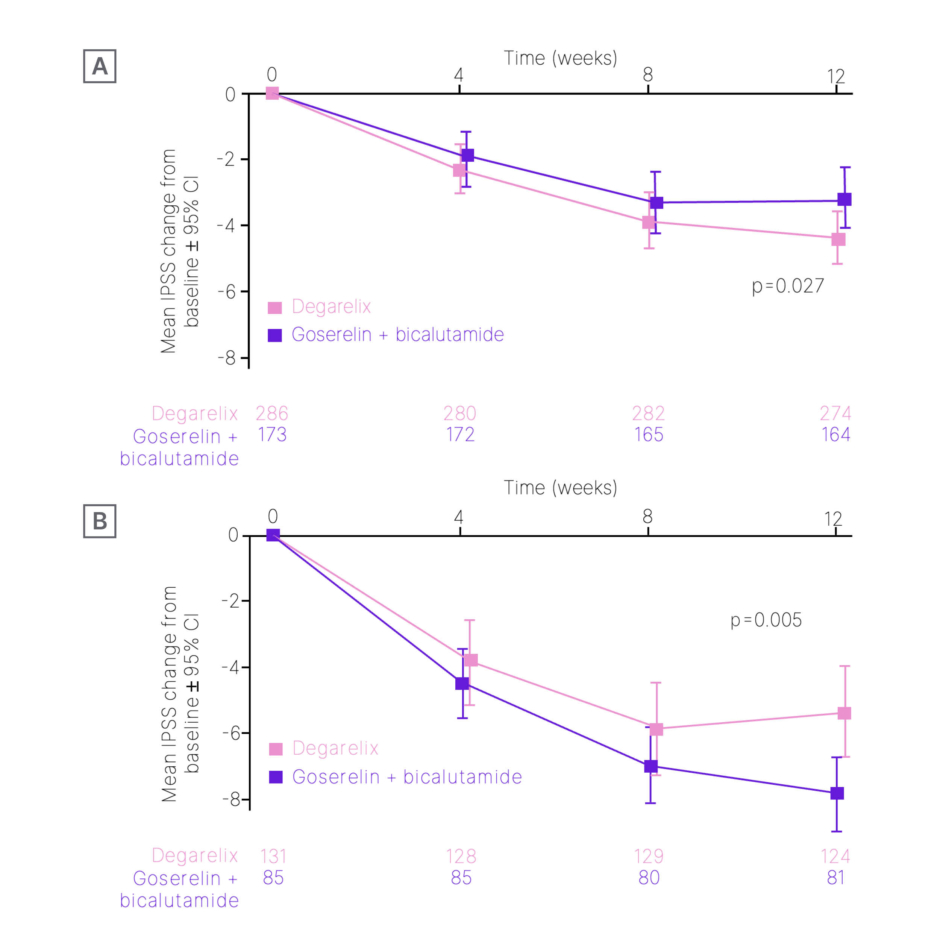
Figure 2: Longitudinal adjusted mean change in IPSS in all patients (A) and patients with IPSS ≥13 at baseline (B).10
Adapted from Mason M et al.10
IPSS: International Prostate Symptom Score.
Testosterone Suppression and Recovery
Briganti concluded his talk by discussing testosterone suppression and recovery with GnRH antagonists compared with agonists, showing the HERO trial data, which demonstrated the superior rapidity and depth of testosterone suppression with relugolix compared with leuprolide.6 By Day 4, mean testosterone levels had declined to 38 ng/dL in the relugolix group, compared with 625 ng/dL in the leuprolide group. By Day 15, 98.7% of patients in the relugolix group had achieved testosterone levels below 50 ng/dL, versus 12% of patients receiving leuprolide. The primary endpoint of sustained castration rate from Day 29 to Week 48 was achieved in 96.7% of patients receiving relugolix and 88.8% with leuprolide, demonstrating the noninferiority of relugolix versus leuprolide (difference: 7.9 percentage points; 95% CI: 4.1–11.8; non specified superiority; p<0.001; Figure 3).6
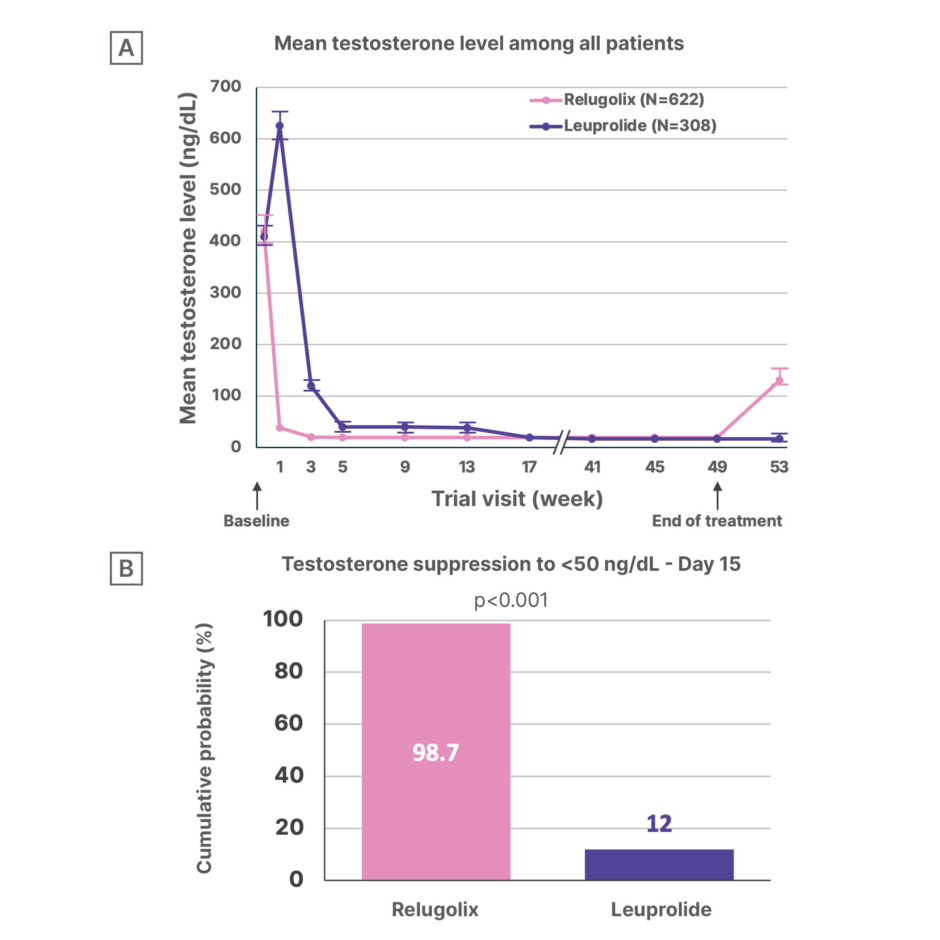
Figure 3: HERO study: Testosterone suppression with relugolix versus leuprolide.6
Adapted from Shore N et al.6
A) Depicts mean testosterone levels over time, including testosterone recovery after 30 days discontinuation of trial treatment at the end of Week 48.
B) Depicts the cumulative probability of testosterone suppression to <50 ng/dL on Day 15.
In a subgroup analysis, testosterone recovery following treatment discontinuation was also markedly superior with relugolix.6 At Day 90 after stopping treatment, mean testosterone levels were 288.4 ng/dL in the relugolix group compared with 58.6 ng/dL in the leuprolide group, with 54% of relugolix-related patients recovering to ≥280 ng/dL versus only 3% of those who had received leuprolide (nominal p=0.002).6 Briganti explained that this has important implications for patients who may require treatment interruption or who are planned for short-course ADT in combination with radiotherapy.
Injectable ADT: The Foundation of Care in Advanced Prostate Cancer in the USA
Scott B. Sellinger, Advanced Urology Institute, Tallahassee, Florida, USA, opened his session by providing a historical and scientific foundation for ADT in prostate cancer. He traced the field from the seminal work of Charles Huggins, whose research in the 1940s demonstrated that androgen withdrawal produced catastrophic effects on prostate cancer, ultimately leading to him receiving the Nobel Prize in 1966, to the current era of diversified ADT options.12
Sellinger presented an overview of the mechanisms of androgen pathway inhibition, encompassing surgical castration (bilateral orchiectomy), GnRH agonists, GnRH antagonists, and androgen receptor pathway inhibitors. He emphasised that ADT remains the foundation of care for prostate cancer across the treatment continuum, from localised disease in combination with radiotherapy through to metastatic castration-resistant prostate cancer.13,14
ADT Choices in 2026
Sellinger provided a comprehensive overview of available luteinising hormone-releasing hormone agonist therapy options in 2026, including leuprorelin mesylate, leuprolide acetate, triptorelin pamoate, and goserelin. Drawing on comparative data from key clinical trials, he outlined the efficacy of 6-month injectable GnRH agonist formulations, noting that published data for each achieved castration testosterone serum levels of ≤50 ng/dL in 93% of patients, with sustained castration maintained through the duration of the respective study periods.15-17
Sellinger noted that bilateral orchiectomy achieves rapid testosterone reduction, with mean time to castrate levels of approximately 8.6 hours, and remains cost-effective over time, but is irreversible and increasingly uncommon in contemporary practice. Data from US Veterans Affairs (VA) registry studies highlight that all forms of medical and surgical castration are associated with increases in metabolic comorbidities, including diabetes, coronary artery disease, myocardial infarction, stroke, and sudden cardiac death compared with no ADT, reinforcing the importance of baseline risk assessment irrespective of the ADT modality chosen.18-20
A Ready-To-Use 6-Month Leuprorelin Formulation
Sellinger focused in depth on leuprorelin mesilate injectable suspension, a ready-to-use, pre-filled 6-month formulation of leuprorelin that received marketing authorisation from the EMA in May 2022 and FDA approval in May 2021.21,22 Unlike other leuprorelin formulations that require reconstitution prior to administration, leuprorelin mesilate is provided as a single sterile pre-filled syringe administered subcutaneously every 6 months, eliminating the preparation steps associated with traditional depot formulations.23
A Phase II, open-label, multicentre study assessed leuprorelin mesilate in patients with advanced prostate cancer. Leuprorelin mesilate was shown to be effective in achieving testosterone suppression to castrate levels (≤50 ng/dL) by Day 28 in 98.5% of subjects, and two doses (6 months apart) successfully suppressed the serum testosterone to castrate levels in 97.6% of subjects (Figure 4).23 Sustained testosterone suppression from Day 28 through Day 336 was achieved in 97.0% of patients.23 In addition to deep and sustained testosterone suppression, leuprorelin mesilate demonstrated a reduction in prostate-specific antigen (PSA) levels, with more than 90% of subjects experiencing a decrease in PSA levels on Day 28. The safety profile of leuprorelin mesilate was consistent with the known class effect of GnRH agonists.23
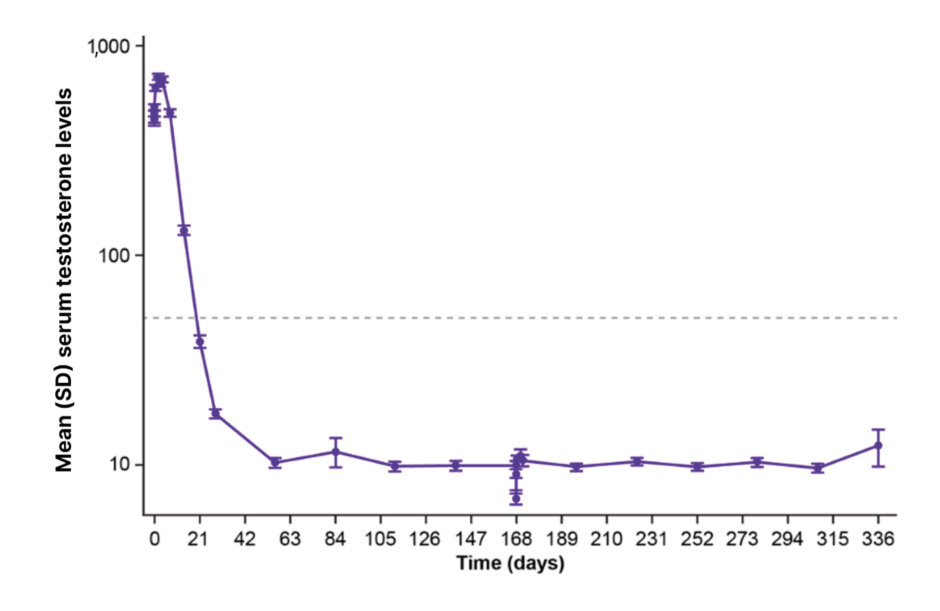
Figure 4: Mean serum testosterone over time in the ITT population.23,a
aThe ITT population was defined as any subject who received at least one dose of leuprorelin mesilate and the PP population was defined as any subject who received two doses of leuprorelin mesylate, followed the inclusion/exclusion requirements of the protocol, and had no major protocol violation. The ITT and PP populations were used in the efficacy analyses. Any subject receiving a dose of leuprorelin mesilate 50 mg was included in the safety analysis.
Adapted from Shore N et al.23
ITT: intention-to-treat; PP: per protocol.
Sellinger highlighted a significant unmet clinical need for ready-to-use injectable formulations. He explained that the reconstitution processes for multi-step depot formulations carry a risk of preparation error, potential for suboptimal castration from inadequate mixing, and increased resource utilisation for nursing staff and healthcare systems.24 The ready-to-use nature of leuprorelin mesilate addresses these practical barriers, which Sellinger identified as particularly relevant in USA urology practices.
Panel Discussion
Following the final presentation, an open panel discussion moderated by Juan Gomez-Rivas, Hospital Clinico San Carlos, Madrid, Spain; and Hilary Glen, Beatson West of Scotland Cancer Centre, Glasgow, UK, gave attendees the opportunity to have their questions answered by the experts. Briganti began by addressing a question on what patients should be screened for CV risk. Briganti explained that patients who are candidates for long-term ADT should be discussed in a multidisciplinary setting. In his centre, patients would be seen upfront by a cardiologist to assess CV status, even those planned for short-term ADT; however, he acknowledged this may not always be possible in different centres. Regardless, he recommended that all patients be seen by a cardiologist even if further down the line.
Briganti and Glen emphasised that risk mitigation strategies are pivotal but not often carried out or suggested to patients, including lifestyle changes such as no smoking and physical activity, which, although seem ‘basic’, can have a significant impact on CV outcomes when a patient is on long-term ADT. Glen added that in these patients who are at increased risk of CVD, the data and guidelines show that a GnRH antagonist should be considered over a GnRH agonist.
Regarding testosterone escapes, Sellinger mentioned that he checks testosterone levels every time he checks PSA levels. If a patient’s testosterone levels are rising while on ADT, the question becomes whether the patient is becoming castration resistant or if there is an issue with the medication, either from the medication not having been administered correctly or non-adherence.
Gomez-Rivas concluded the symposium by asking each speaker to summarise their key takeaways, with Sellinger highlighting that risk mitigation is an important strategy that needs to be worked on, especially for high-risk patients, and as clinicians we should be proactive as opposed to reactive with regard to CV risk. Briganti emphasised that patients should be screened for baseline CV risk before treatment initiation and choose the appropriate ADT therapy based on each individual patient profile. Glen closed the session by noting that, based on current guideline discussions and emerging clinical evidence, GnRH antagonists may be considered as a treatment option in patients with a history of CVD or an elevated CV risk, alongside an individualised assessment of overall patient factors.
Conclusion
The selection of ADT in prostate cancer continues to evolve in response to a growing evidence base, greater appreciation of patient comorbidities, and the expanding range of available treatment options. A key development has been the introduction of both injectable and oral GnRH antagonists, which offer rapid and sustained testosterone suppression without the initial testosterone surge associated with GnRH agonists, thereby eliminating the need for concurrent antiandrogen use to prevent initial testosterone surge. This symposium brought together expert faculty to explore how individual patient characteristics, including CV history, LUTS burden, disease setting, and practical treatment considerations, should inform ADT selection.
The panel reinforced a consistent message across specialities: proactive CV risk assessment, not reactive management, should underpin ADT decision-making. Clinicians should screen for baseline CV risk prior to treatment initiation and select ADT therapy according to the individual patient profile. Patients with a history of CV events, at high CV risk, or with clinically significant LUTS should be considered for a GnRH antagonist, with particular urgency in settings such as impending spinal cord compression, where rapid testosterone suppression is critical.
| Adverse events should be reported. For UK healthcare professionals, reporting forms, and information can be found at https://yellowcard.mhra.gov.uk/. Adverse events should also be reported to Accord-UK LTD on 01271 385257 or email [email protected]. For non-UK/EU healthcare professionals, you can report side effects directly via the national reporting system listed in Appendix V of the EU SmPC. |






