INTRODUCTION
Sodium hypochlorite (NaOCl), the active ingredient in household bleach, has long been a staple in medical history, yet its full potential in dermatology remains underexplored. A 2025 scoping review by Chang et al.1 synthesized available literature, analyzing 222 studies from 1915–2024 to map NaOCl’s past applications, current evidence, and future directions (Figure 1). This feature appraises that review, critically examining established knowledge while highlighting NaOCl’s relevance in modern contexts and suggesting areas for future advancements. Originally referred to as Dakin’s solution, NaOCl was used during World War I to irrigate infected wounds. In an era before antibiotics, NaOCl played an important role in reducing sepsis and saving limbs on the front lines due to its low cost, broad antimicrobial spectrum, and unique ability to dissolve necrotic tissue. Its use faded when penicillin was introduced in the 20th century, and it became referred to as outdated and irritative. However, among rising antibiotic resistance and new research exploring its anti-inflammatory mechanisms, the use of NaCOl has been rediscovered in recent decades.
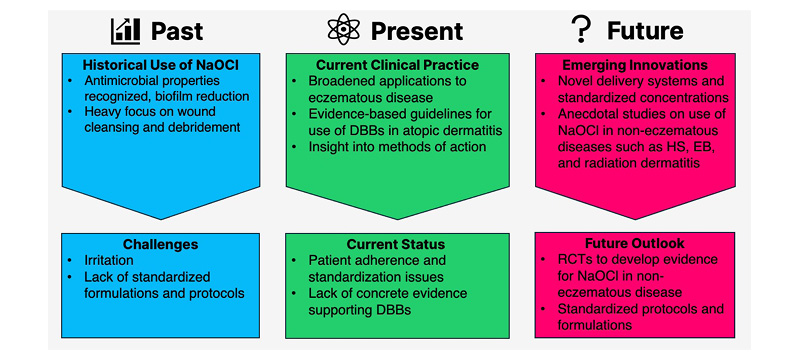
Figure 1: The evolving landscape of NaOCL in dermatology.
DBB: dilute bleach bath; EB: epidermolysis bullosa; HS: hidradenitis suppurativa; NaOCl: sodium hypochlorite.
HISTORICAL PERSPECTIVES AND MODERN MECHANISTIC INSIGHTS
Initially, the success of Dakin’s solution was attributed to mechanical debridement, but research later showed that the chemical composition of NaOCl played a role in sloughing of necrotic skin to facilitate healing. When in an aqueous solution, NaOCl and hypochlorous acid (HOCl) are at an equilibrium. A lower, more acidic pH favors a shift toward HOCl with more potent antimicrobial and cytotoxic effects. Therefore, it is important that the pH of NaOCl solutions used for medical purposes is regulated to confer a balance between antimicrobial and toxic effects that can be corrosive to healthy cells. These findings were initially highlighted in studies from the 1960s and 70s, which focused on optimizing the balance between NaOCl and HOCl to maximize efficacy and minimize cytotoxicity. A key finding was dose-dependent effects and trade-offs to treatment. The highest dose may not be the most effective dose due to increased risk for adverse reactions including skin irritation, fibroblast damage, contact dermatitis, and patient discomfort. Antimicrobial properties against Staphylococcus aureus and Pseudomonas aeruginosa could be harnessed with concentrations of 0.005–0.5% NaOCl, incurring a lower risk for side effects.1 This review highlights how historical insights paved the way for the modern, broader application of NaOCl, though inconsistencies in preparation (e.g., household bleach strength, dilution methods, and storage) still hinder comparability and the development of specific guidelines for use in evidence-based medicine. Early studies were often observational or in animal models, limiting translation but establishing NaOCl’s application beyond antiseptics.1
KEY FINDINGS AND EVIDENCE
The scoping review organized evidence into four clinical domains, revealing robust support for NaOCl across dermatoses. By synthesizing information based on date and domain, this review effectively summarized historical perspectives, current patterns, and future directions. Additionally, domains with limited research could be highlighted. Among the 222 articles included for review, 57 described antimicrobial properties, 64 wound care, 78 eczematous skin disease, and 23 non-eczematous inflammatory skin conditions.1 Direct grading of the quality of evidence was not included in the original review.
Antimicrobial Properties
Antimicrobial properties take precedence in early literature, describing broad-spectrum activity against bacteria, fungi, viruses, and parasites. The largest breadth of studies focused on common skin pathogens like S. aureus (including methicillin-resistant strains), P. aeruginosa, and Candida species. However, a wide variety of pathogens were targeted, including herpes simplex virus, Streptococcus spp., Enterococcus spp., Escherichia coli, dermatophytes, Morganella morganii, Enterobacter cloacae, Klebsiella pneumoniae, Malassezia spp., Sporothrix schenckii, Aspergillus spp., and even maggots like Lucilia sericata. Antimicrobial effects were evaluated using bacterial cultures and a wide range of concentrations from as low as 0.000025% to 10%.1-3 Not only did concentration affect outcomes, but longer exposure times were found to increase the efficacy of more diluted solutions. Cell toxicity has been a consistent concern, and, most recently, concentrations under 0.05% have been favored to avoid skin irritation, although doses as low as 0.005% have shown antimicrobial effects. Factors like solution pH, age, and the skin’s natural barriers affect real-world performance.1
Wound Care
NaOCl’s capacity to disrupt biofilms and multidrug-resistant organisms has been established in chronic wounds and burns. Outside of its role in infection control, NaOCl can positively affect wound healing across multiple stages. Low concentrations have been found to facilitate debridement by softening necrotic tissue, reduce excessive neutrophil activation that may prolong inflammation, increase or sustain fibroblast activity, and stimulate granulation tissue. While higher concentrations are typically associated with negative effects, one in vivo model found that 4% NaOCl promoted angiogenesis.1 Clinical reports show faster ulcer closure and fewer amputations in diabetic foot cases, though evidence is mixed for burns, with some trials noting discomfort or graft sloughing at higher doses.1 It is important to note that the benefit of NaOCl in wound care and as an antimicrobial agent is dependent on dose, exposure time, and pathogen strain. A study comparing 0.1% and 0.5% NaOCl-soaked gauze for maintenance of burn wounds found that while 0.5% NaOCl was effective in eradicating S. aureus and P. aeruginosa, it could not be used for more than 2 weeks continuously due to epidermal toxicity.2 Comparatively, 0.1% NaOCl was able to reduce microorganisms with no epidermal damage but needed to be used for a longer period.2 Further studies are needed to elucidate the exact role and precise concentrations of NaOCl required to optimize wound healing.1
Eczematous Skin Disease
Most literature regarding NaOCl use in eczematous conditions is centered on atopic dermatitis (AD). Dilute bleach baths (DBB; often approximately 0.005% NaOCl) have been used as an adjunctive treatment option for moderate-to-severe AD colonized by S. aureus. The objective of DBBs is to decolonize S. aureus and reduce the incidence of skin and soft tissue infections. However, recent studies highlight inconsistent results and question the validity of DBBs.1,4,5 Meta-analyses found no superiority over plain water for severity scores like Eczema Area and Severity Index (EASI) or body surface area.1,4,5 Additionally, there is no standardized dilution formulation for DDBs, and the household use of DBBs poses significant heterogeneity, as bath tub sizes vary.1
Emerging data suggest direct anti-inflammatory effects via inhibition of the nuclear factor κB pathway, which, when activated, promotes pro-inflammatory cytokine production, T cell activation, and histamine release.6 This mechanism is likely why DBBs can ease symptoms like redness, itching, and skin barrier issues in AD, even when bacterial reduction is inconsistent. This study highlights that NaOCl’s benefits go beyond killing bacteria and emphasizes its broader therapeutic value.
Non-eczematous Disease
Non-eczematous applications are the newest and smallest area of research. Emerging areas of study include reduction in the severity of radiation dermatitis, improved desquamation in rare ichthyoses, infection prevention in epidermolysis bullosa and hidradenitis suppurativa (HS), and papule reduction in acne vulgaris. These findings underscore NaOCl’s versatility, but the review justly critiques the predominance of case reports and observational data, with heterogeneity confounding meta-analyses.1
DISCUSSION
The review’s strengths lie in its comprehensive nature, including historical perspectives, novel applications, and critical lens on the strength (or lack thereof) among cited literature. Limitations include the exclusion of studies with a focus on HOCl, comparative studies using another component in combination with NaOCl, and non-English language publications. Due to these exclusion criteria, there may be other applications and mechanisms on NaOCl not included in the scoping review. Additionally, specific clinical protocols and evaluation of evidence strength remain lacking. All things considered, the importance of NaOCl was well-described across multiple applications. Among the ever-changing medical landscape, NaOCI addresses enduring concerns regarding antibiotic resistance and resource limitations. It remains a viable treatment option in guidelines from the USA, Canada, Europe, and Asia, which endorse its use in DBBs for moderate-severe AD, though consensus on mild cases or exact dosing is lacking.1,7
FUTURE DIRECTIONS
Despite a lengthy history, clinical application of NaOCl has ample room for innovation to determine the optimal concentrations and formulations to use in each setting: antimicrobial, anti-inflammatory, and wound healing (Table 1). Prioritizing dosing to maximize effectiveness in each unique setting may be the future, rather than the current one-bathtub-fits-all application. Standardized formulations, such as pH-buffered cleansers or sprays, can mitigate instability, enhance compliance, and bypass variability. This benefit is highlighted by commercially available NaOCl cleansers, which exemplify this approach and have shown practical utility in the management of eczematous skin disease.10 Comparative trials pitting NaOCl against HOCl, biologic therapies, and examining a combination approach would clarify mechanisms and offer better guidance for personalized regimens.1
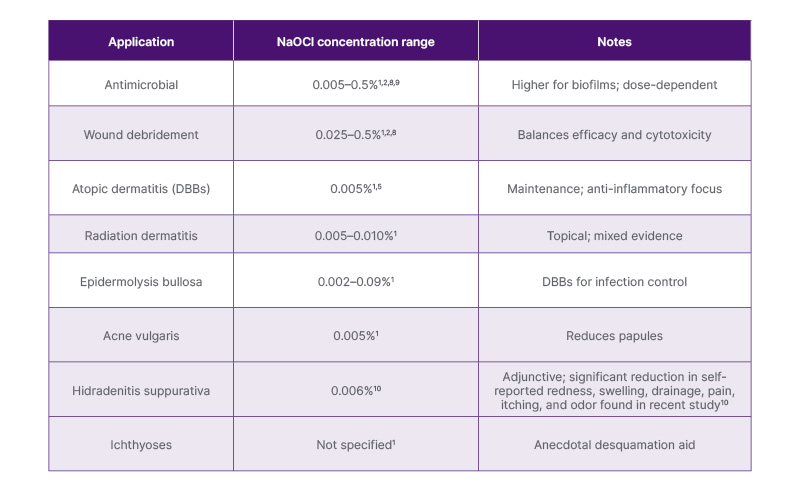
Table 1: Current recommended NaOCl concentrations by dermatologic application.1-3,5,8-10
Concentrations adapted from multiple supporting studies.1-3,5,8-10
DBB: dilute bleach bath.
In non-eczematous realms, RCTs for HS, radiation dermatitis, epidermolysis bullosa, and rare ichthyoses could validate anecdotal benefits and stimulate development of standard guidelines. This process has already begun, as evidenced by a recent study using a NaOCl body wash of standardized concentration (0.006% NaOCl; CLn® BodyWash, TopMD Skin Care, Dallas, Texas, USA) for HS management.8 This uncontrolled study demonstrated significant reductions in HS symptoms, illustrating the potential of standardized NaOCl formulations while underscoring the need for future RCTs to confirm these findings and strengthen the evidence base. Advancing standardized protocols and innovative delivery systems through RCTs will be essential to unlock NaOCl’s full therapeutic potential and establish clear, evidence-based roles across dermatologic indications.1
CONCLUSION
NaOCl embodies dermatology’s blend of tradition and innovation, representing an accessible, promisingly effective, and yet under-optimized therapeutic approach. Chang et al.1 charts a path forward to make what is old new, urging refinement of protocols and expansion of trials. Currently, NaOCl is clinically used for wound debridement; viral, bacterial, and fungal infections; and as an adjunct treatment for AD. Further studies are needed to determine standardized dilution and the role of NaOCl in non-eczematous cutaneous disease. By bridging gaps in evidence, NaOCl could reclaim its place as a reliable and highly utilized therapy, offering safe, equitable solutions in an era of complex skin conditions.





