BACKGROUND AND AIMS
Extramammary Paget’s disease (EMPD) is a rare intraepithelial adenocarcinoma that typically arises in apocrine gland-rich areas such as the vulva, scrotum, and perineum. Clinically, EMPD often presents as a chronic, pruritic, erythematous plaque that can mimic benign dermatologic conditions, frequently leading to delays in diagnosis and treatment.1 Despite its often indolent appearance, EMPD is associated with high recurrence rates and, in some cases, underlying malignancy, making optimal management critical.2
MATERIALS AND METHODS
Surgical excision remains the standard of care. Historically, wide local excision (WLE) has been the primary treatment modality.3 However, its effectiveness is limited, contributing to high rates of positive margins and recurrence.4,5 Mohs micrographic surgery (MMS), in contrast, allows for complete margin assessment through staged excision with real-time histologic evaluation, offering improved tissue conservation and lower recurrence rates. Prior studies have demonstrated recurrence rates of approximately 7–22% with MMS compared to 26–33% with WLE, supporting MMS as a superior approach in appropriately selected patients.6,7
Despite this evidence, treatment patterns for EMPD remain highly variable across specialties. The authors’ recent single-center case series of 23 patients with biopsy-confirmed EMPD demonstrated that both referring and treating specialty significantly influenced surgical management decisions.8 Dermatologists were the only providers performing MMS, while gynecologic oncology and obstetrics/gynecology specialists exclusively utilized excisional approaches such as WLE or vulvectomy. Notably, no patients referred by gynecologic oncology or obstetrics/gynecology underwent MMS, highlighting a lack of cross-specialty referral even when evidence supports its use.
RESULTS
These findings suggest that EMPD management may be driven more by specialty-specific practice patterns than by evidence-based decision-making. This discrepancy has important clinical implications. In the authors’ cohort, recurrence rates were higher among patients treated with traditional excisional approaches compared to those undergoing MMS, consistent with existing literature (Figure 1). Persistent reliance on WLE in certain specialties may therefore contribute to increased recurrence, repeat procedures, and patient morbidity.
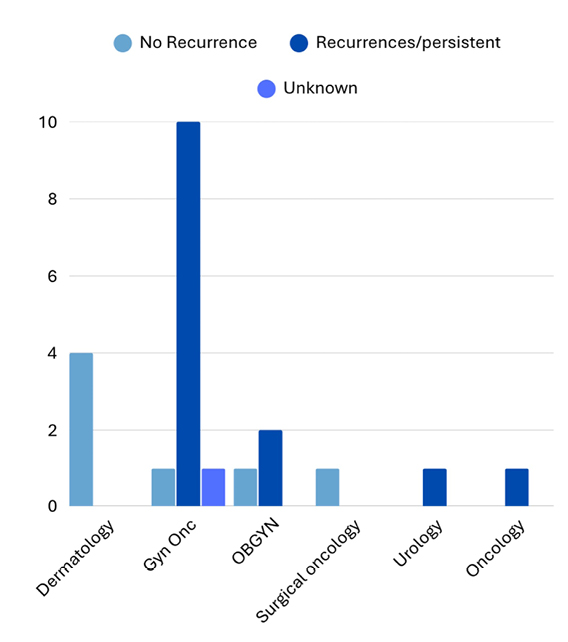
Figure 1: Recurrence rates by treating specialty in patients with extramammary Paget’s disease.
Note that one patient did not have treatment after diagnosis.
Gyn Onc: gynecologic oncologist; OBGYN: obstetrician-gynecologist.
Several factors likely contribute to these patterns, including limited access to MMS outside of dermatology, established referral networks that reinforce specialty-specific care pathways, and the absence of consensus treatment guidelines for EMPD. Without standardized recommendations, treatment decisions may default to provider familiarity rather than comparative outcomes data.
A multidisciplinary approach is essential to optimize EMPD management. Improved collaboration between dermatology, gynecologic oncology, and surgical oncology may facilitate appropriate patient selection for MMS and reduce recurrence rates. Additionally, the development of standardized referral pathways and increased awareness of MMS outcomes among non-dermatologic providers could help address existing gaps in care.
CONCLUSION
In conclusion, although MMS demonstrates superior outcomes for EMPD, its utilization remains limited by specialty-driven practice patterns. Addressing these disparities through multidisciplinary collaboration and guideline development is critical to improving outcomes in this rare malignancy.





