Interview Summary
Chronic inflammatory demyelinating polyneuropathy (CIDP) is a rare, severe, and progressive immune-mediated disease characterised by predominant demyelination of motor and sensory nerves, which can lead to potentially irreversible nerve damage and long-term disability due to weakness and sensory ataxia. Despite available standard-of-care treatments, many patients experience suboptimal responses, relapses, or treatment burden, highlighting the need for new, targeted therapeutic options. Increasing evidence supports a critical role for pathogenic IgG autoantibodies in the pathogenesis of CIDP, and a shift toward treatments that target underlying disease biology rather than symptom control alone. By targeting neonatal Fc receptor (FcRn), efgartigimod alfa enables selective reduction of pathogenic immunoglobulin G (IgG), representing a mechanism-driven therapeutic approach.In the global Phase II ADHERE trial, the FcRn blocker, efgartigimod alfa, demonstrated clinical efficacy, reducing relapse risk and improving disability scores.
During interviews conducted by EMJ, two internationally recognised experts in neurology, Thomas Skripuletz, Senior Neurologist and Professor of Neurology at Hannover Medical School in Germany; and Charulatha Nagar, Adult Neurologist and Clinical Assistant Professor of Neurology at Northwestern Medicine’s Feinberg School of Medicine in Chicago, Illinois, USA, explored their clinical practice experience using efgartigimod alfa to treat patients with CIDP. Experts discussed how clinical evidence from the ADHERE trial and real-world experience with efgartigimod alfa underpins real-world treatment decision-making, and provided practical insights to support neurologists considering efgartigimod alfa for their patients with CIDP.
IgG AUTOANTIBODIES PLAY A KEY ROLE IN CIDP
CIDP is a rare, severe, and progressive autoimmune neuropathic disease that can cause irreversible nerve damage, resulting in disability due to limb weakness, sensory disturbances, fatigue, and sometimes pain.1-5 It can lead to functional disability or sensory deficits, with patients often reporting problems with mobility, balance, and fatigue.2-6 Consequently, CIDP is associated with a substantial clinical burden and can negatively impact patients’ daily activities, work productivity, and health-related quality of life.4-8
Despite available traditional treatments, many patients experience suboptimal responses, relapses, or treatment burden, highlighting the need for new, targeted therapeutic options. This ongoing unmet need is further underscored by real-world data from a Dutch registry, where although 97% of patients received treatment, 88% still reported residual symptoms, including pain (52%) and fatigue (77%).9-11
The pathophysiology of CIDP is complex, evolving, and heterogeneous, reflecting the involvement of multiple cellular and humoral immune mechanisms that may vary between patients. Emerging evidence suggests that IgG autoantibodies may play a key role.5,12 IgG autoantibodies are considered to contribute to demyelination in CIDP in 2 ways: (1) Macrophage recruitment when IgG anchors to the myelin sheath, meaning macrophages may recognise and bind to the Fc portion of the IgG and phagocytise the myelin; and (2) IgG-mediated complement activation where complement proteins may recognise and bind to IgG anchored on the myelin sheath, activating the complement pathway and ultimately recruiting more macrophages (Figure 1).13
“The introduction of FcRn-blockers represents a new targeted approach, focusing on the reduction of circulating IgG antibodies,” Skripuletz elaborated. “From a neurological perspective, this development is interesting because it reflects an evolving understanding of the role of pathogenic IgG antibodies in at least a subgroup of CIDP patients.”
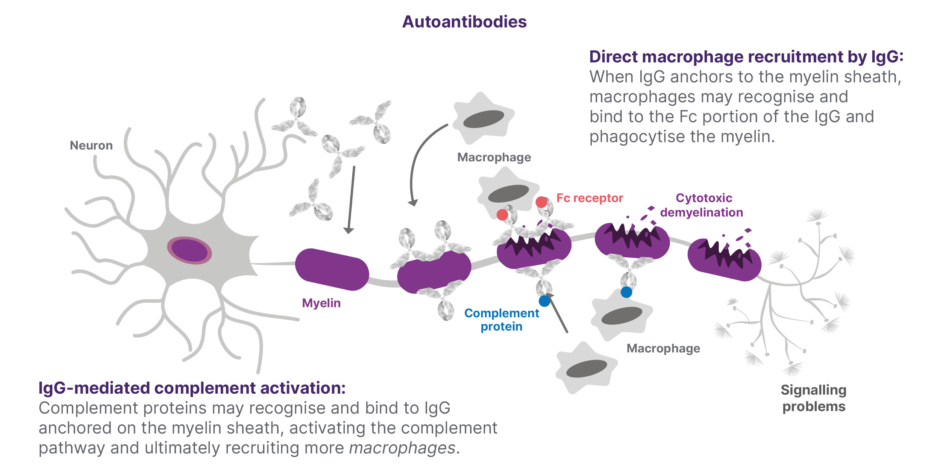
Figure 1: The role of IgG autoantibodies in demyelination in CIDP13
Adapted from Querol et al.13
EFGARTIGIMOD ALFA: A NOVEL TARGETED THERAPY IN CIDP
Recent therapeutic innovations, including the introduction of subcutaneous immunoglobulins, have already contributed to reducing the disease burden in CIDP.14,15 However, despite these advances, there remains a substantial unmet need for additional treatment options. Although treatment approaches in CIDP have evolved over recent decades, disease management has still largely relied on broad immunomodulatory therapies such as glucocorticoids, off-label immunosuppressive therapies, or human plasma-derived immunoglobulins, without specifically targeting the underlying disease mechanisms.10
Despite these approaches, important treatment gaps remain. Not all patients respond adequately to current therapies, which may also be associated with side effects and treatment burden that can negatively impact work productivity and quality of life. Real-world and published data suggest that approximately 20-30% of patients do not respond adequately to first-line therapies, and around 15% remain treatment-refractory, underscoring the limitations of existing options and the need for more effective, targeted treatments.16,17
Efgartigimod alfa is a human IgG1 antibody fragment that selectively blocks the neonatal Fc receptor and results in targeted reduction of IgG levels, without impacting IgG production, other immunoglobulins, or reducing albumin levels like full-length antibody-based FcRn blockers.1,12,18,19 Efgartigimod alfa subcutaneous was evaluated clinically in the Phase II, double-blind, placebo-controlled ADHERE study, supporting the key role of IgG in CIDP (studied in 322 patients with active disease).12 In this pivotal study, efgartigimod alfa subcutaneous showed improvements in disability and strength in patients with CIDP, and significantly reduced the risk of relapse compared to placebo in those who responded to treatment.12
In the ADHERE trial, efgartigimod alfa subcutaneous was also well-tolerated in patients with CIDP, and the majority of treatment-emergent AEs, including infections, were mild or moderate in severity.12 As Nagar confirmed: “Efgartigimod alfa has an acceptable safety profile that has already been consistently demonstrated across multiple clinical trials and further supported by real-world experience in other indications, such as myasthenia gravis, with over 7 years of clinical and real-world experience in more than 10,000 patients.20,21 It is generally well-tolerated in clinical trials, which reinforces confidence in its safety and aligns with the positive experiences reported by patients.”12,18
Based on the results from the ADHERE trial, efgartigimod alfa subcutaneous is now approved for CIDP in several countries worldwide, including the USA and Japan, and indicated in the EU as monotherapy for the treatment of adults with progressive or relapsing active chronic CIDP after prior treatment with corticosteroids or immunoglobulins.1,21-23
Given the unmet needs that exist in the current clinical practice, management of CIDP, and the lack of treatment innovation over recent decades, both experts welcomed the introduction of new targeted therapeutic options such as efgartigimod alfa.
“Glucocorticoids and intravenous immunoglobulin (IVIg) are effective treatments, particularly in the early phases of CIDP,” explained Skripuletz. “However, up to 30–50% of patients do not respond adequately or show only a partial response. In addition, some patients who initially respond may experience clinical worsening over time, requiring treatment escalation,’’ he added. “For these reasons, several gaps remain in the management of CIDP,” Skripuletz continued. “Treatment responses can be variable and sometimes unpredictable. Some patients require increasingly frequent treatment intervals to maintain stability, while others experience only partial benefit.
“Against this background, it is encouraging that additional therapeutic options are becoming available,” commented Skripuletz. “This is particularly relevant for patients who do not respond or do not respond adequately to immunoglobulins or glucocorticoids, or who continue to deteriorate despite ongoing treatment. Expanding the range of treatment strategies may help us better individualise therapy and address the heterogeneous nature of CIDP,” he added.
Nagar described efgartigimod alfa as a novel targeted FcRn-based approach to CIDP treatment that has been “very well studied and backed up by the ADHERE trial.”12 She also pointed out that efgartigimod alfa marks the first innovative mechanism for CIDP treatment “in decades.”15
RAISING THE BAR IN CIDP TREATMENT GOALS
“In my clinical practice as a neurologist, CIDP is a relatively frequent immune-mediated neuropathy that we see both in specialised neuromuscular clinics and in general neurology practice,” Skripuletz observed. “Patients often present with progressive weakness, sensory loss, gait instability, and impaired hand function, which can significantly affect daily activities and quality of life.”15
Treatment goals in CIDP, according to European Federation of Neurological Societies/Peripheral Nerve Society (EFNS/PNS) 2021 guidelines, include reducing disease activity, improve or stabilise neurological function, prevent disability progression, and maintain long-term functional independence while minimising treatment-related burden.24
Both experts stressed the importance of timely diagnosis, early initiation of effective therapy, and thoughtful sequencing of treatments in CIDP to help prevent ongoing nerve damage and reduce the long-term burden of disability. Traditional approved treatment options include glucocorticoids, immunoglobulin (administered either intravenously or subcutaneously), and plasma exchange or immunoadsorption.15 These treatment approaches are largely empirical, in that their main goal is to reduce or suppress clinical symptoms by modulating or dampening down the immune system.2,15 Clinical evidence also indicates that a proportion of patients do not respond to these treatments, and persistent disease activity may remain despite ongoing therapy.12,25
“From a clinical perspective, this highlights the importance of having additional therapeutic options available to help achieve treatment goals,” Skripuletz emphasised. “Expanding the treatment landscape allows neurologists to better individualise therapy and adapt treatment strategies to the heterogeneous course of the disease and the needs of individual patients.”
“For patients, the most important goal of treatment is to prevent functional disability, especially in patients that are diagnosed and treated early. For patients that have progressed despite early treatment with IVIg and/or glucocorticoids, the question has been whether new targeted treatments like efgartigimod alfa can restore functional ability. That would significantly raise the bar in the treatment of CIDP, even if this would only occur in a small group of patients with CIDP,” said Nagar.
REAL-WORLD PATIENT CASES WITH EFGARTIGIMOD ALFA RESTORING FUNCTIONAL ABILITY
As experts outlined, real-world use of efgartigimod alfa has been informed by clinical experience from the ADHERE study.12
Discussing results from the pivotal ADHERE trial, Nagar noted that “66% of patients achieved confirmed evidence of clinical improvement in strength and/or functional ability. Approximately 40% of them showed a very early clinically meaningful improvement by week 4.’’12 This variability in response timing and magnitude highlights the need for ongoing monitoring, she explained, together with management of patients’ own treatment expectations.
“Continued treatment with efgartigimod alfa was associated with a 61% relative reduction in relapse risk versus placebo, which is a very important point,” Nagar emphasised.12 “What we are trying to do is keep patients from experiencing the recurrent relapses that may become long-term disability.”
Experts were asked to share case study examples from their own clinical practice where efgartigimod alfa played a meaningful role in managing CIDP. Nagar outlined real-world experiences from her neurology practice that highlight the meaningful impact of transitioning patients with CIDP from conventional therapies, such as IVIg and other immunomodulatory treatments, to efgartigimod alfa. As she explained: “We’re looking for something that’s a little bit easier on them and in hopes of improving their disabilities, and that’s been my experience with efgartigimod alfa.”
Patient Case 1: The Business Owner – Progressing 5 Years On IVIg
One particularly striking case involved a patient she had treated with IVIg for approximately 5 years. Despite initial management, the patient (who owned a catering business) experienced a steady functional decline that increasingly limited his ability to continue the work he loved. “We decided, it’s time for a change,” she recalled. After switching to efgartigimod alfa subcutaneous, the patient showed gradual improvement, and about a year into treatment, he was able to resume his business. For Nagar, this moment was especially powerful: “When I saw the patient back, that was a really incredible moment, being able to help someone return to something they truly loved.”
Patient Case 2: The Hands-On Crafts Enthusiast – Wheelchair Bound for 3 Years
She shared another deeply personal case of a man in his 70s, a crafts enthusiast, who had slowly progressed to a wheelchair over 3 years. Previously diagnosed with CIDP, he had tried IVIg but discontinued treatment due to adverse effects and remained untreated for several years despite meeting diagnostic criteria. When he initiated efgartigimod alfa subcutaneous, the results were transformative. About a year and a half later, he regained enough function to return to crafting. Nagar described the emotional impact of this recovery: “He actually brought in his work and I saw what he had made. That’s what made it real.”
These cases, she emphasised, reflect a broader therapeutic goal informed by both clinical trial evidence, such as the ADHERE study, and real-world experience. “We’re not looking at complete resolution of the disease,” she noted. “We are making meaningful improvements, reducing relapses, and preventing the accumulation of disability, using something that’s more efficacious for them.”
In both patients, the transition to efgartigimod alfa not only stabilised disease progression but also restored independence and quality of life, enabling them to return to the activities that defined their sense of purpose. However, responses to treatment may vary, and not all patients experience similar outcomes.
Patient Case 3: Patient In Their Late 60s with Waning Effect Between IVIg Infusions
Skripuletz described the case of a patient diagnosed with CIDP 14 years earlier who initially responded well to IVIg after opting against glucocorticoids. Early treatment led to meaningful improvements in motor and sensory symptoms, allowing the patient to maintain independence with only minor limitations for several years.
After approximately 8 years, however, the duration of benefit between IVIg infusions began to decline. Although dose adjustments provided some improvement, the waning effect persisted. The patient was subsequently transitioned to subcutaneous immunoglobulin (SCIg), which offered greater stability and reduced symptom fluctuations, though with a slightly less pronounced overall effect. A later dose increase helped maintain temporary stability.
Over time, the patient experienced a gradual deterioration in walking ability and reduced walking distance, reflecting a progressive loss of treatment efficacy. As Skripuletz emphasised, this case highlights a common clinical challenge: patients who initially respond well to immunoglobulin therapy but experience diminishing benefit over time, underscoring the need to reassess treatment strategy and consider alternative options.
Despite the increasing physical limitations, the patient remained grateful for the years of disease stabilisation achieved with immunoglobulin therapy. At the same time, he became increasingly concerned about future disease progression and the possibility of losing further mobility and independence. These concerns played an important role in the shared decision to transition to efgartigimod alfa.
This patient is currently still in the early phase following treatment transition. According to Skripuletz, the patient has already reported a slow but steady increase in muscle strength and an improvement in walking distance. Although long-term outcomes remain to be determined, these early changes have been perceived positively by the patient and have contributed to renewed optimism regarding disease control and preservation of independence.
Given the historical reliance on a limited number of therapies, treatment escalation or switching in CIDP was often deferred, even in the presence of suboptimal response. The introduction of targeted options such as efgartigimod alfa allows clinicians to reconsider this paradigm and potentially switch earlier to optimise outcomes.
Patient Case 4: Loss Of Clinical Effect with IVIg
This patient developed numbness in the feet and hands, followed by weakness predominantly affecting the feet, resulting in reduced walking speed and later a limitation in walking distance. Initially, the hands were only mildly affected, but over time, weakness also developed. Because the patient also reported joint pain, a trial of low-dose prednisolone was initiated. However, this had no effect on either the weakness or the joint symptoms. In addition, side effects occurred, and prednisolone treatment was therefore discontinued. Approximately 2 years later, the diagnosis of CIDP was established, and treatment with immunoglobulins was started. Initially, the patient responded to immunoglobulin therapy, with improvement in walking ability. Unfortunately, after a few months, a decline became apparent again. The immunoglobulins had no relevant effect on hand function. Treatment was subsequently switched to efgartigimod alfa subcutaneous. An improvement in strength and function of the feet became evident within the first 4 weeks. Further improvement was observed over the following weeks. Now, half a year after treatment initiation, the patient is not symptom-free but has achieved improved function compared with the previous condition, making it possible to walk longer distances again and to go hiking. He trains extensively and remains hopeful for further improvement.
PRACTICAL ADVICE FOR USING EFGARTIGIMOD ALFA: HOW TO INITIATE TREATMENT AND MONITOR
To aid physicians in incorporating efgartigimod alfa into routine care, a recently published expert consensus guidance (2025), developed by German specialists including Skripuletz himself, offers practical recommendations on patient selection and treatment transition, including use of a 1-week regimen.26 “In daily practice, the transition from immunoglobulins or glucocorticoids needs to be carefully planned in order to avoid gaps in disease control,” Skripuletz explained. “Therefore, an individualised plan for gradual dose reduction and eventual discontinuation should be discussed with the patient. Efgartigimod alfa subcutaneous should preferably be initiated before the clinical effect of current CIDP therapies starts to decrease.”1
“When we looked at the timing of the switch, we chose this interval because IgG serum levels rise very quickly after an IVIg infusion, but then decline again, with a substantial proportion already decreasing by approximately 50% within the first week after treatment. Thereafter, serum IgG levels continue to decline, although at a considerably slower rate,” Skripuletz explained. “This means that the week following an infusion represents the period of maximum immunoglobulin effect. Starting efgartigimod alfa too early, when IgG levels are still very high, could therefore amount to overtreatment. On the other hand, waiting too long to initiate treatment may expose some patients to unnecessary clinical deterioration due to the delayed onset of action. The goal is to find the right balance and ensure a seamless transition, although clinical judgment remains essential,” he continued.
This rationale aligns with the German expert consensus guidance (2025) on the use of efgartigimod alfa in CIDP, which recommends initiating efgartigimod alfa 7 days after the last IVIg infusion, based on IgG kinetics and clinical experience to optimise treatment continuity and avoid both overtreatment and clinical deterioration.26 “Patients who have previously been treated with glucocorticoids cannot discontinue this therapy abruptly. Patients who have been treated with regular plasma exchange or immunoadsorption can usually be transitioned to the efgartigimod alfa within a few days after the last apheresis procedure.”
Both experts emphasised the importance of close patient monitoring in the initial period after switching therapy. “Patients should be carefully assessed during the first four weeks,” Skripuletz suggested.
Although the timing of switching to efgartigimod alfa was not studied in the ADHERE trial, Nagar confirmed that “there is a Phase IV study looking at the switch 1 week from the use of IVIg.” This open-label, multicentre study will evaluate the proportion of patients transitioning from IVIg to efgartigimod alfa who are still receiving efgartigimod alfa at the end of the 12-week treatment period.27
Nagar confirmed that efgartigimod alfa plays a key role in current CIDP management and noted that its introduction is starting to reshape the treatment landscape. “Therapies targeting FcRn represent an additional treatment option within the broader CIDP management strategy,” Skripuletz agreed. “CIDP is a heterogeneous disease, and no single therapy is effective for all patients,” he added.
Both experts agreed that treatment success with efgartigimod alfa subcutaneous should combine clinical metrics with individual patient perspectives, particularly regarding the disease’s impact on day-to-day quality of life. “Treatment success should be assessed using objective clinical scores that are recommended in established diagnostic and monitoring criteria for CIDP,” emphasised Skripuletz. “In addition, the patient’s own perception of improvement plays an important role in evaluating treatment benefit.”
Nagar explained how improvements in clinical scores can translate into meaningful everyday gains, showing that “patients are getting better.” For example, improved grip strength in the hands means patients can hold their toothbrush or brush their hair, while improved endurance scores can enable patients to get rid of their cane, or walk instead of using a wheelchair. These improvements are “so important to patients,” she stressed.
As Nagar pointed out, treatment success with efgartigimod alfa may be reflected not only by functional improvement, but also disease stabilisation and prevention of clinical deterioration. She therefore educates patients that efgartigimod alfa may not provide complete resolution of symptoms, but is intended to “reduce relapses, which are associated with progressive disabilities in some patients.”
“Careful monitoring of treatment response in patients receiving IVIg is essential and should include both clinical assessments and patient-reported outcomes. In cases of insufficient or waning response, timely reassessment and consideration of alternative therapeutic strategies, including approaches such as efgartigimod alfa, may support improved disease control,” said Skripuletz.
Experts outlined several assessment tools that can be used to monitor patients and assess treatment efficacy in real-world practice, including objective impairment measures such as grip strength, disability measures like the Inflammatory Neuropathy Cause And Treatment (INCAT) score, the Medical Research Council (MRC) sum score, and the Inflammatory Rasch-Built Overall Disability Scale (I-RODS), as well as walking assessments to evaluate gait speed and endurance.28
Among these, grip strength represents a particularly practical and sensitive measure that can be assessed frequently in routine clinical care and closely reflects patients’ functional ability in daily activities.24,29,30 “I track the grip strength, the endurance, i.e., walking improvements and the ability to do more daily activities, and the INCAT scores or the I-RODS scores to see the meaningful changes that patients are making,” Nagar explained.
This approach is aligned with current guidelines, which recommend using at least one disability measure (e.g., INCAT or I-RODS) and at least one impairment measure. Grip strength offers a simple, reproducible tool to monitor treatment response over time, while patient-reported outcomes provide essential context.24
In the ADHERE study, 40% of patients experienced an early and clinically meaningful improvement by Week 4.12 However, Nagar pointed out that the timing of response to efgartigimod alfa can vary among patients; a longer treatment period may be needed to assess therapeutic effectiveness.
In terms of early indicators of treatment response, Skripuletz highlighted “improvement in muscle strength, better walking ability, or increased endurance in daily activities. Some patients also report reduced sensory symptoms or improved stability during walking,” he added.
Nagar pinpointed improvements in endurance and dexterity as key markers of early response, such as the ability to walk a few more steps or handle small buttons on clothing. “A small response might be identified very early on but still becomes a very meaningful response as we go forward,” she noted.
Experts highlighted the importance of regular and structured assessment of treatment response over time. Skripuletz suggested that response should be evaluated within the first 3 months to guide ongoing treatment decisions, while Nagar noted that some patients may demonstrate continued or delayed improvements, supporting reassessment over a longer timeframe of up to 6 months.
In terms of monitoring frequency, experts advised that patients are reassessed regularly during initial efgartigimod alfa treatment cycles, then at defined intervals depending on the clinical course, typically every 3 months.
Both experts also highlighted the importance of careful monitoring in patients who are temporarily off treatment. Some patients may remain clinically stable for prolonged periods after successful treatment and subsequent discontinuation of therapy. However, even in apparently stable patients, regular reassessment remains essential, as CIDP may reactivate and lead to renewed accumulation of disability if clinical deterioration is not recognised early. Clinical evaluation should be considered 3 to 6 months after treatment initiation to assess the treatment effect and at regular intervals thereafter.1 Objective clinical measures together with patient-reported symptoms can help identify early signs of relapse and support timely re-initiation of therapy.
Identifying Suitable Candidates for Efgartigimod Alfa
Discussing target patient profiles, experts agreed that efgartigimod alfa may be considered in patients with progressive or relapsing active CIDP following prior treatment with corticosteroids or immunoglobulins, particularly where disease control is suboptimal, unstable, or associated with treatment burden.
Patients with fluctuating or insufficient disease control on IVIg or glucocorticoids
Efgartigimod alfa may be considered in patients with ongoing disease activity despite standard therapy, including those experiencing: end-of-dose deterioration (clinical worsening before the next IVIg dose); need for shortened IVIg intervals or dose escalation to maintain stability; or progressive or persistent symptoms (e.g., reduced hand grip strength, walking impairment) impacting daily function.
“In clinical practice, I would mainly consider efgartigimod alfa for patients with active CIDP who have not achieved satisfactory disease control with standard first-line treatments,” explained Skripuletz.
Patients with clinically relevant side effects
Patients experiencing treatment-related burden or tolerability issues may also be appropriate candidates, including side effects from long-term glucocorticoid use alone or in combination with IVIg treatment, challenges associated with frequent IVIg infusions or plasma exchange, or difficulty maintaining treatment schedules due to lifestyle or comorbidities.
Severe complications during treatment with immunoglobulins are rare overall, and most patients tolerate therapy well. Nevertheless, some patients may develop intolerances such as skin rashes or headaches. In the OPTIC trial, combined treatment with IVIg and intravenous methylprednisolone was associated with an increased incidence of thromboembolic events, raising safety concerns regarding the combined exposure to immunoglobulins and glucocorticoids.31 The authors reported that: “Safety concerns associated with combined IVIg and intravenous methylprednisolone must be resolved before its potential benefits in improving disability and impairment can be implemented in clinical practice.”
These factors may therefore prompt consideration of alternative, more manageable treatment approaches.
Patients with disease recurrence after treatment discontinuation
Some patients may discontinue prior therapy (e.g., IVIg, SCIg, or glucocorticoids) and remain stable for a period; however, CIDP remains a progressive disease with ongoing risk of relapse. Patients who become symptomatic again after treatment discontinuation, or require re-initiation of immunomodulatory therapy, may benefit from a re-evaluation of treatment strategy, including consideration of targeted options.
Patients with insufficient response, seeking reduced treatment burden and greater independence
Beyond efficacy, treatment convenience and quality of life are important considerations. Efgartigimod alfa may be particularly relevant for patients requiring frequent infusion-based therapies, experiencing logistical and time burden, or preferring at-home, self-administered treatment options.
“For some patients, the option of self-injection reduces the need for frequent hospital visits and allows treatment to be integrated more easily into daily life,” noted Skripuletz.
Nagar highlighted that weekly at-home administration may better align with patients’ daily routines and reduce disruption.
“The key point is that treatment decisions should remain individualised and based on the clinical course, treatment response, and patient preferences,” stressed Skripuletz.
SUMMARY
Finally, experts were asked to provide their key advice for neurologists considering efgartigimod alfa for patients with CIDP. “Efgartigimod alfa is a targeted, plasma-free product that is available in the toolbox for CIDP management,” Nagar summarised, highlighting its ease of use, favourable safety and tolerability profile, and ability to reduce relapse risk versus placebo.
“Based on my clinical experience, efgartigimod alfa represents a new treatment option, particularly for patients with ongoing disease activity or insufficient response to standard therapies,” explained Skripuletz. “It is important to monitor patients closely and assess response early, and where appropriate, not delay optimisation of therapy. In selected patients, this may include earlier switching to improve disease control and reduce the risk of ongoing nerve damage.”
“At the same time, treatment of CIDP remains complex, and no single therapy is effective for all patients,” he added. “There are still individuals who do not respond sufficiently to IVIg, SCIg, glucocorticoids, or efgartigimod, which highlights the continued need for additional therapeutic options. It is therefore encouraging that further clinical studies are ongoing to evaluate new treatments with different mechanisms of action.”
| Adverse events can be reported to [email protected] or by using the local medical information telephone number. You will find these in the package leaflet of the SmPC. Adverse event reporting details can also be found here. |
EU-VYV-26-00016 © argenx BV | Date of preparation: June 2026