Abstract
Hyponatraemia is the most common electrolyte abnormality among hospital inpatients. This retrospective cohort study examined demographic characteristics, diagnostic investigations, clinical management, and outcomes of patients admitted with severe hyponatraemia (serum sodium ≤120 mmol/L) over an 18-month period.
A total of 202 patients were admitted with severe hyponatraemia. Hypertonic saline (HS) was administered to 25.2% of patients, and was associated with rapid correction (>8 mmol/L/24 hours) in 31.4% of recipients. The overall rate of rapid correction was 28.2%.
18-month mortality was 40.1%, rising to 50% among patients with no correction at 24 hours. Hypertonic saline use was associated with reduced mortality (27.5% versus 44.4%; p=0.03). No patients died from hyponatraemic encephalopathy, or from complications associated with rapid correction. Readmission within 6 months was common (31.2%), with recurrent hyponatraemia in 60.3% of these cases. One case of osmotic demyelination syndrome occurred in association with rapid correction.
This study demonstrates the poor prognosis associated with severe hyponatraemia, with substantial morbidity and mortality observed at 18 months.
Key Points
1. Severe hyponatraemia was associated with an 18-month mortality of 40.1%, rising to 50% among patients who failed to show any sodium increase within the first 24 hours. Hospital readmissions, frequently with recurrent hyponatraemia, and new long-term care needs, were also common.2. No deaths were attributed to hyponatraemic encephalopathy or complications of rapid correction, indicating that excess mortality is driven by the underlying cause of hyponatraemia rather than the condition itself.
3. Long-term morbidity and mortality related to severe hyponatraemia remain under-recognised, and it should be considered a marker of poor prognosis reflecting serious underlying disease.
INTRODUCTION
Hyponatraemia is the most common electrolyte abnormality among hospital inpatients, with clinical manifestations ranging from asymptomatic disease to life-threatening conditions.1 Its aetiology is diverse and is often classified according to the clinician’s assessment of extracellular fluid volume status. Severe hyponatraemia may present with neurological features such as confusion, seizures, and coma, collectively referred to as ‘hyponatraemic encephalopathy’, which requires urgent treatment with hypertonic saline (HS).2 However, rapid correction of chronic hyponatraemia carries the risk of osmotic demyelination syndrome (ODS), a rare but serious neurological disorder.2
ODS, formerly known as central pontine myelinolysis, was first described by Adams et al.3 in 1959 as a neurological condition manifesting as pseudobulbar palsy and quadriplegia occurring in chronic alcoholics. Liver disease, alcohol use, hypokalaemia, and malnutrition are known risk factors for ODS, with rapid correction of chronic hyponatraemia also proposed in the 1980s.4 Sterns et al.5 in 1986 suggested that ODS is a preventable complication of overly rapid correction of chronic hyponatraemia based on observations of eight patients with hyponatraemia admitted over a 5-year period who had a worsening neurological condition after rapid correction. Incidence of ODS in a large multicentre study of 22,858 patients with hyponatraemia was 0.05%, with a frequency of rapid correction of 17.7%, although this population also included patients with mild hyponatraemia (plasma sodium [pNa]<130 mmol/L).6
Mortality associated with hyponatraemia has been well documented. In 1984, Baran et al.7 reported a mortality rate of 27% among hospitalised patients with hyponatraemia, with highest mortality at 64% in those with central nervous system symptoms related to factors other than hyponatraemia. A more recent longer-term prospective study observed a substantial 12-month mortality of 20.6% in patients with pNa less than 125 mmol/L. Rehospitalisation incidence in this group was also high at 56.2%, with recurrent hyponatraemia in 42.7%.8 Mortality rates exceeding 50% have been observed in some populations with pNa less than 120 mmol/L after a median follow-up of 431 days.9
Despite these findings, the reported mortality rates in severe hyponatraemia remain variable, and the cause of death is often unrelated to hyponatraemia itself. Chawla et al.10 observed only three deaths over a 12-year period that were directly attributed to hyponatraemic encephalopathy, with highest inpatient mortality associated with severe progressive illness such as sepsis or multiorgan failure. Underlying medical comorbidities associated with a high Charlson’s risk index are more likely to be associated with death in hyponatraemic patients, rather than severity of hyponatraemia itself.11
Analogous patterns are seen in other conditions. For example, hip fractures are associated with a well-recognised 1-year mortality of around 30%.12 The leading causes of death in this group include circulatory disease, dementia, and malignancy, suggesting that poor prognosis reflects the underlying frailty and comorbidities predisposing to fracture, rather than the fracture itself.13
The primary aim of this study is to compare management strategies and correction rates in a population with severe hyponatraemia, and to evaluate their impact on long-term outcomes, particularly 18-month mortality.
METHODS
Data from inpatients with severe hyponatraemia (serum sodium ≤120 mmol/L) between 1st February 2022–31st July 2023 were retrospectively analysed. Cases were identified from laboratory records of all hyponatraemia events during this 18-month period. Both Emergency Department and inpatient cases were included. Duplicate entries were removed, but readmission events were documented. Outpatient cases and likely spurious sodium readings were excluded. A total of 202 patients were included in the final analysis.
Demographic data, diagnostic evaluations, therapeutic interventions, and sodium correction rates were reviewed. Correction rates were based on pNa 24 hours after the preceding measurement, with rapid correction defined according to hospital protocol as an increase >8 mmol/L within 24 hours.
Long-term outcomes, including readmission (within 6 months) and 18-month mortality rates, were recorded. Discharge destination was included if a new long-term care requirement arose during the index hospital admission.
Subgroup analyses focused on specific management strategies (e.g., HS use or management in critical care environment), rapid correction (>8 mmol/L in 24 hours), and extreme hyponatraemia (serum sodium ≤110 mmol/L). Categorical variables were compared using Pearson’s χ2 test or Fisher’s exact test where expected cell counts were <5. Statistical significance was defined as p<0.05.
RESULTS
Cohort Characteristics
Among 202 patients, the median age was 68 years (range: 16–95 years), with a balanced sex distribution (50.5% male). Common aetiologies included hypovolaemia (22.3%), syndrome of inappropriate antidiuretic hormone (21.8%), and hypervolaemia (17.3%). Alcohol-related hyponatraemia accounted for 12.4% of cases, while 6.4% (n=13) had extreme hyponatraemia (pNa ≤110 mmol/L). Mixed aetiology was observed in 8.9%, which was defined as presence of more than one concurrent mechanism of hyponatraemia, as diagnosed by the treating physician. Demographic characteristics of the study population are displayed in (Table 1).
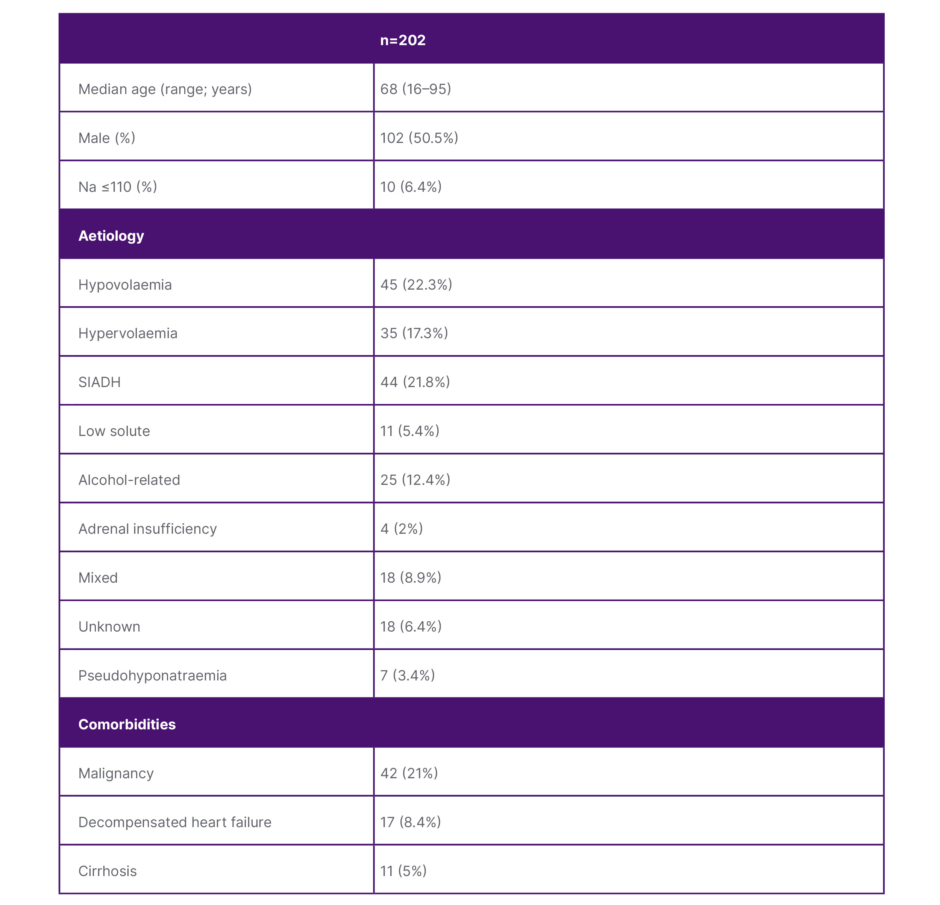
Table 1: Demographic characteristics
Na: sodium; SIADH: syndrome of inappropriate antidiuretic hormone.
True hyponatraemia (serum osmolality <285 mmol/kg) was observed in 78.2%, while pseudohyponatraemia was rare (3.4%; n=7). Diagnostic work-up revealed high urine osmolality (>300 mmol/kg) in almost 50%, while urine osmolality was low (<100 mmol/kg) in only 5%. Urine sodium <20 mmol/L and urine sodium >40 mmol/L was noted in 41.1% and 25.7%, respectively. Urine diagnostic studies (urine sodium or urine osmolality) were tested in 176 patients (87%). Thyroid dysfunction and adrenal insufficiency were uncommon contributors. While syndrome of inappropriate antidiuretic hormone was commonly diagnosed (21.8%), a culprit medication was documented in only four patients, all of whom were prescribed selective serotonin reuptake inhibitors, serotonin and norepinephrine reuptake inhibitors, or carbamazepine/oxcarbazepine. Medication-related hyponatraemia was also observed in patients prescribed thiazide diuretics, resulting in cessation of this drug in six patients, along with loop diuretics in four patients, and mineralocorticoid receptor antagonists in two patients.
MANAGEMENT
HS was administered to 25.2% of patients, primarily in critical care settings (92.2%). Rapid sodium correction (>8 mmol/L/24 hours) occurred in 31.4% of HS patients versus 27.2% of non-HS patients (p=0.56), while safe correction rates (≤8 mmol/L/24 hours) were also similar between these groups (39.2% versus 34.4%; p=0.54). Sodium correction rates by HS use are displayed in (Table 2).
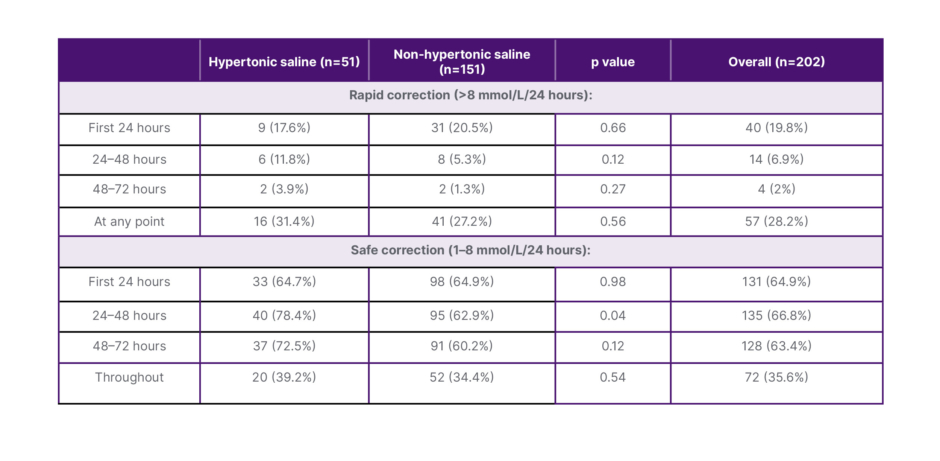
Table 2: Sodium correction rates by hypertonic saline use.
(Table 3) demonstrates clinical characteristics, aetiology, management, and outcomes according to hyponatraemia correction rate in the first 24 hours of diagnosis only. Group 1 did not increment, or had a decline in pNa in the first 24 hours of diagnosis, whilst Groups 2 and 3 had slow (1-8 mmol/L/24 hours) or rapid (>8 mmol/L/24 hours) correction, respectively.
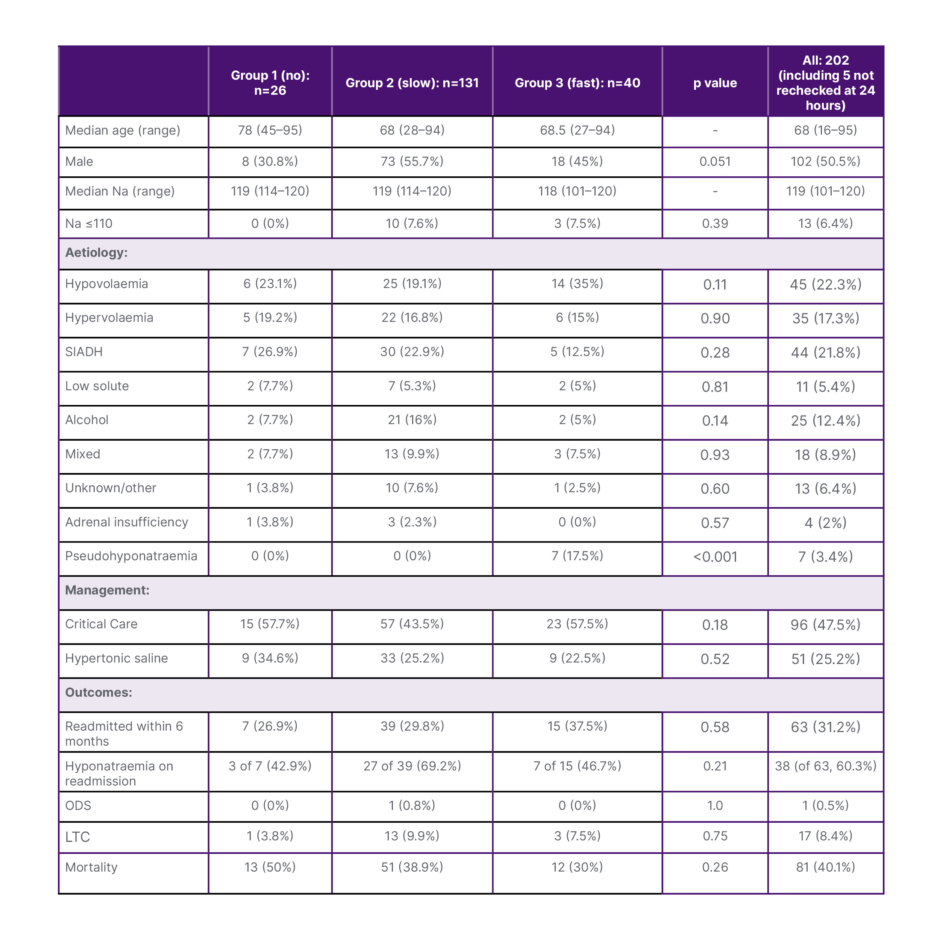
Table 3: Clinical characteristics, aetiology, management, and outcomes according to hyponatraemia correction rate in the first 24 hours of diagnosis.
LTC: long-term care; Na: sodium; ODS: osmotic demyelination syndrome; SIADH: syndrome of inappropriate antidiuretic hormone.
Rapid correction of pNa in any 24 hour period in the first 72 hours of diagnosis was observed in 28.2%, with clinical characteristics detailed in (Table 4). Notably, mortality was lower in those who experienced rapid correction (26.3% versus 45.5%; p=0.02).
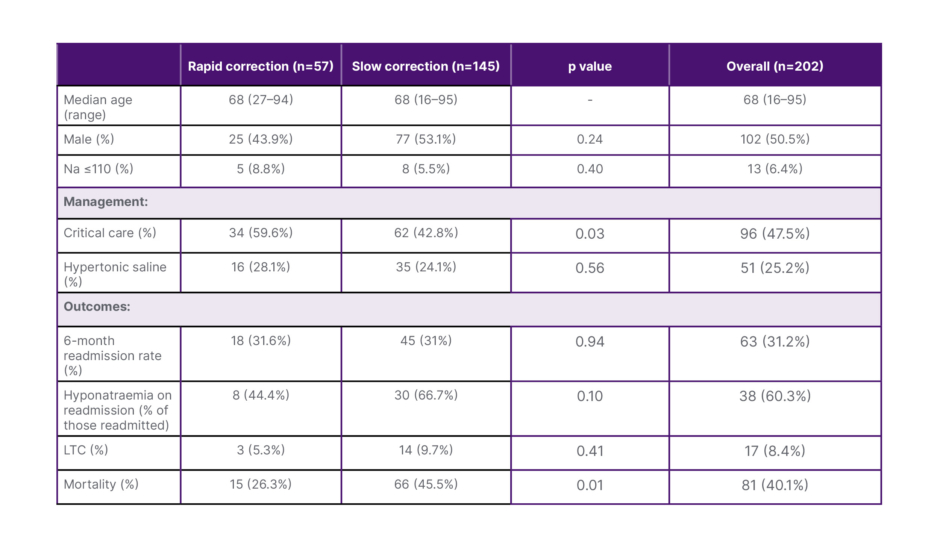
Table 4: Rapid (>8 mmol/L/24 hours) versus slow correction (1–8 mmol/L/24 hours) of sodium after 72 hours.
LTC: long-term care; Na: sodium.
Patients with extreme hyponatraemia (pNa ≤110 mmol/L) were more likely to require critical care management (92.3% versus 44.4%; p=0.001), and receive HS (84.6% versus 21.2%; p<0.001). An increased frequency of alcohol-related causes was observed in this group, though not reaching statistical significance (23.1% versus 11.1%; p=0.63).
In addition to use of HS, other treatment strategies included use of intravenous crystalloids in 102 patients (50.5%), and fluid restriction in 91 patients (45%). Loop diuretics were prescribed in 35 patients (17.3%), and sodium chloride tablets in 33 (16.3%). Prescription of multiple therapies (e.g., fluid restriction and loop diuretic) was common, and many patients had changes to therapy during their treatment course. Rescue strategies for rapid correction of plasma sodium included intravenous hypotonic fluid use, typically with 5% dextrose solution, or administration of desmopressin. Despite the incidence of rapid correction of 28.2%, the frequency and choice of rescue strategy use was not accurately recorded.
Outcomes
The overall 18-month mortality was 40.1% (n=81). As displayed in (Table 3), the highest frequency of mortality was observed among patients with no correction at 24 hours (Group 1, 50%), followed by those with slow correction (Group 2, 38.9%) and rapid correction (Group 3, 30%), though not reaching statistical significance (p=0.26). Mortality was similar in the extreme hyponatraemia group at 23.1% compared to 41.3% in the pNa 111–120 mmol/L group (p=0.25).
Of patients who died during their index hospitalisation with hyponatraemia, hyponatraemic encephalopathy or complications of hyponatraemia correction were not documented as cause of death in any cases. Common causes of death were malignancy in 35 patients (43.2%), decompensated cirrhosis in seven (8.6%), and decompensated heart failure in seven (8.6%).
Patient outcomes associated with use of HS are displayed in (Table 5). Mortality was lower among patients who were treated with HS compared to non-HS management (27.5% versus 44.4%; p=0.03), but overall re-admission rates (25.5% versus 33.1%; p=0.31) were similar. The readmission rate within 6 months was 31.2%, with recurrent hyponatraemia in 60.3% of these cases. Re-admission with hyponatraemia was observed more frequently among patients who were previously treated with HS (84.6% versus 54%; p=0.04). Long-term care requirements arose in 8.4% of patients, reflecting the chronic impact of severe hyponatraemia.
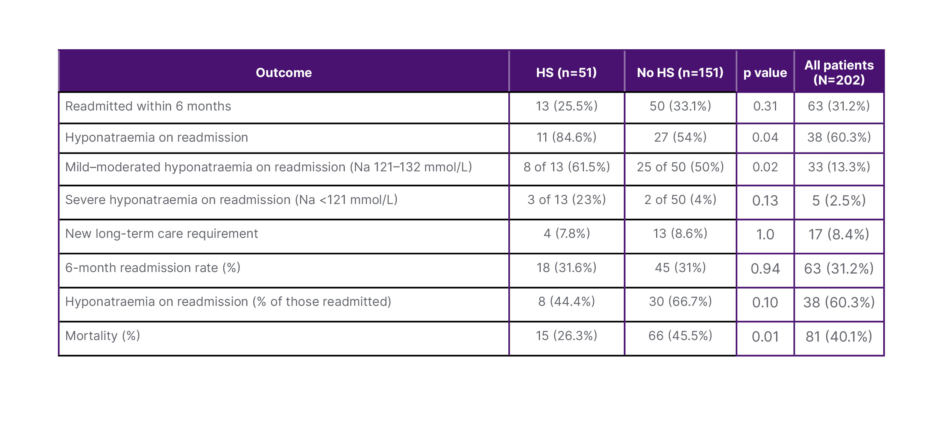
Table 5: Outcomes according to use of hypertonic saline.
HS: hypertonic saline; Na: sodium.
One case of ODS occurred in association with rapid correction in a 68 year-old male admitted with symptomatic hyponatraemia of 113 mmol/L, with past medical history notable for significant alcohol consumption. This patient was managed with intravenous isotonic saline and did not receive HS. An increase in plasma sodium of 7 mmol/L was observed in the first 24 hours, 10 mmol/L in the second 24 hours, and 6 mmol/L further between hours 48–72. MRI was consistent with ODS, and he made a full neurological recovery.
DISCUSSION
Severe hyponatraemia management requires a balance between timely correction and avoidance of complications like osmotic demyelination. Many patients require management in a critical care environment, and the observed rapid correction rate of 28.2% in this cohort highlights the need for close monitoring.
HS appears beneficial when judiciously applied, with a lower mortality rate observed in this cohort. Incidence of rapid or safe correction was similar in HS recipients compared to non-HS management. Readmission with hyponatraemia was commonly observed, and often with severe hyponatraemia again.
HS has emerged as a treatment standard in cases of symptomatic hyponatraemia to prevent neurological complications such as hyponatraemic encephalopathy, with a goal to increase pNa by 4–6 mmol/L in the first 4 hours.14 The HS administration rate of 25.5% in cases of severe hyponatraemia observed in this cohort reflects under-utilisation of HS in the authors’ centre. Correction limits are suggested to reduce the risk of iatrogenic brain injury secondary to rapid correction, and desmopressin is proposed as a mechanism to prevent water diuresis.15 Varying approaches of proactive (in anticipation of water diuresis), reactive (in response to water diuresis), or rescue (rapid correction has already occurred) strategies to desmopressin administration have been described, but a clear consensus has not been reached.15
MacMillan et al.16 retrospectively analysed 1,450 admissions with severe hyponatraemia and compared correction strategies according to desmopressin use, concluding that a reactive approach resulted in improved safe sodium correction. In contrast to this, AlShanableh et al.17 observed improved rates of overcorrection in patients treated with a proactive desmopressin approach along with HS administration, compared to a reactive or rescue approach in a smaller observational study of patients with severe hyponatraemia. Many experts still propose a proactive strategy to desmopressin use, along with HS administration, which may reduce the incidence of overcorrection in severe hyponatraemia at risk for ODS.15,18,19
A limitation of the authors’ study was that rescue strategies such as use of hypotonic fluids or desmopressin were not recorded. This was also a single centre, retrospective, observational analysis of HS prescribing practices, whereas prospective data collection would be beneficial. Several subgroup analyses were limited by small sample sizes and sparse event frequencies, reducing statistical power, and the heterogenous presentations of hyponatraemia represent challenges in clearly classifying disease aetiology.
The most striking observation in this study was the 18-month mortality of 40.1% among patients with severe hyponatraemia, rising to 50% in those who failed to demonstrate any increment in sodium within the first 24 hours. However, no patients in the study died of hyponatraemic encephalopathy, or from complications associated with rapid correction. This suggests that the underlying aetiology of hyponatraemia, particularly those conditions predisposing to slower or more difficult correction, may drive excess mortality rather than the correction process itself.
Patients with the most profound hyponatraemia (pNa ≤110 mmol/L) had reduced mortality, though not reaching statistical significance. Alcohol- and medication-related hyponatraemia were common in this subgroup, which may reflect a population with fewer significant medical comorbidities. By contrast, hypervolaemic hyponatraemia was more common in patients who failed to correct at 24 hours or corrected slowly. Seethapathy et al.20 showed that correction rates below 6 mmol/L per 24 hours are associated with increased 30-day mortality, particularly among patients with cirrhosis, congestive cardiac failure, or metastatic cancer, which may explain this observation.20
In conclusion, this study recognises severe hyponatraemia as a prognostic marker for poor outcomes. In addition to long-term morbidity and mortality, severe hyponatraemia is associated with recurrent hospitalisation and long-term care needs. Mortality reached 50% at 18 months in some subgroups, emphasising the importance of recognising severe hyponatraemia as a marker of underlying disease severity and poor prognosis. HS has emerged as a treatment standard in management of this condition, and the reduced mortality observed in the authors’ cohort is further evidence to support this practice.





