Support: This non-promotional article has been funded and facilitated by Bayer and is intended for healthcare professionals only. This article includes the views, opinions, and quotations as expressed by the symposium speakers.
Chairperson: Andrea R. Genazzani1
Speakers: Rossella E. Nappi,2,3 Claudio N. Soares,4 Michelle Jacobson5,6
1. Department of Clinical and Experimental Medicine, Division of Obstetrics and Gynecology, University of Pisa, Italy
2. Department of Clinical-Surgical, Diagnostic and Paediatric Sciences, University of Pavia, Italy
3. IRCCS San Matteo Foundation, Pavia, Italy
4. Queen’s University School of Medicine, Kingston, Canada
5. Coven Women’s Health, Toronto, Canada
6. Department of Obstetrics and Gynaecology, University of Toronto, Canada
Disclosure: Genazzani has been a member of the speaker’s bureau for Abbott, AlfaSigma, Bayer, Besins Healthcare, Bionorica, Exeltis, Gedeon Richter, Mithra, Organon, Sérélys, Se-cure, Theramex, and Viatris.
Nappi has received consulting fees from Besins Healthcare, Fidia, and Vichy Laboratories; and honoraria from Abbott, Astellas, Bayer Healthcare, Exeltis, Fidia, Gedeon Richter, Ibsa, Merck & Co, Novo Nordisk, Shionogi Limited, Theramex, and Viatris.
Soares has received research grants from Atai Therapeutics, Clairvoyant, Canadian Institutes of Health Research, Diamond Therapeutics, Eisai, Ontario Brain Institute, Ontario Centre of Innovation, Otsuka, and SEAMO; and has been an advisory board member for AbCellera, Astellas, Bayer, Eisai, Idorsia, Lundbeck, and Otsuka.
Jacobson has received research grants from the Canadian Institutes of Health Research and the United States Department of Defense; and consulting fees from AbbVie, AbCellera, Astellas, Bayer, Biosyent, Duchesnay, Eisai, Hologic, Idorsia, Knight, Kye, Lilly, Lupin, Merck, Pfizer, Sanofi, and Searchlight.
Acknowledgements: Writing assistance was provided by Helen Boreham, HB Medical (UK) Ltd, Wetherby, UK.
Disclaimer: The Women’s Health Academy is funded and facilitated by Bayer. All case studies presented are fictitious; patient symptoms may vary. This material is intended for healthcare professionals only.
Keywords: Counselling, hot flushes, individualised care, menopause, quality of life, sleep disturbances, vasomotor symptoms (VMS), Women’s Health Academy.
Citation: EMJ. 2026;11[2]:14-22. https://doi.org/10.33590/emj/755OG471
Meeting Summary
During this symposium at the International Society for Gynecological Endocrinology (ISGE) Annual Congress, leading experts in women’s health and members of the Women’s Health Academy explored the spectrum of menopause symptoms and highlighted the need for an individualised and woman-focused approach to menopause care in clinical practice. The Women’s Health Academy is a multidisciplinary expert group that aims to improve women’s healthcare by advancing education, expanding access to evidence-based resources, and putting women at the centre of care.
Rossella Nappi, Professor at the University of Pavia in Italy, began the session by underscoring the impact of menopause on women’s overall health and quality of life, and the importance of integrated symptom recognition that includes vasomotor symptoms (VMS), sleep, mood, and cognitive function. The expert panel, including Andrea Genazzani, Professor at the University of Pisa, Italy; Claudio Soares, Professor from Queen’s University School of Medicine in Kingston, Canada; and Michelle Jacobson, Assistant Professor from the University of Toronto, Canada, then discussed a selection of fictional patient cases. These cases illustrate the need for consultations centred on women’s goals, expectations, and needs to determine the best path to symptom relief and long-term health outcomes. For clinical practice, the experts recommended adopting a simple three-step approach to menopause counselling: 1) identify key symptoms and concerns; 2) focus on symptom relief; and 3) tailor the approach to the individual patient.
The Women’s Health Academy
This symposium at ISGE was delivered by the Women’s Health Academy, a group comprising over 30 international multidisciplinary experts that is dedicated to improving reproductive health and menopause outcomes for women.1 The Women’s Health Academy is funded and facilitated by Bayer and governed by an independent Executive Committee.
As Nappi explained, the role of the Women’s Health Academy is to champion women’s healthcare, fostering community and knowledge sharing among healthcare professionals and women to shape future directions in care. By prioritising women’s voices, it aims to create an environment in which women feel informed and empowered throughout their lives, from puberty to menopause and beyond. As part of its mission, the Women’s Health Academy seeks to address the issues that restrict women’s access to healthcare, challenge taboos, and support the next generation of healthcare professionals in delivering clinical best practice, including menopause care.1
Menopause Symptoms
Every woman is different, and menopause is a personal experience, stressed Nappi. Women may present with a variety of symptoms, which are sometimes misdiagnosed as being unrelated to menopause and which women themselves may accept as an inevitable part of the ageing process.1,2
Common symptoms of menopause include VMS, e.g., hot flashes during the day and/or night sweats at night, and difficulty sleeping. Vaginal symptoms of menopause such as dryness and painful intercourse can occur. Women can also experience menstrual changes as they move towards menopause, including irregular or abnormal bleeding and heavy bleeding, which may result in iron deficiency and anaemia. Menopause can also be associated with musculoskeletal symptoms such as joint pain and soreness.1,3
Beyond the physical manifestations, menopause is linked to a range of associated psychological symptoms, which may include anxiety, poor memory, inability to concentrate, depressed mood, irritability, decreased sexual desire, sleep dysfunction, and impaired cognitive function (commonly known as brain fog).1,3
The Impact of Menopause
Nappi highlighted how the symptoms of menopause can impose a significant burden on patients.1 An international survey conducted from December 2019–February 2020, which included 2,035 women in Europe, 675 in the USA, and 750 in Japan, all aged 40–65 years, assessed the prevalence of symptoms associated with menopause and their impact on quality of life and daily functioning.4 Women ranked their symptoms on a scale from 0 (not bothersome) to 6 (extremely bothersome), with highly bothersome denoted by a score of 4 or above. VMS and sleep disturbances were identified as among the most common and/or disruptive menopause symptoms in this survey among women from Europe and the USA (Figure 1).1,4 Sleep problems were considered to be a highly bothersome menopause symptom, with a ranking of 4.4 in Europe and 4.3 in the USA. Hot flushes or flashes, the hallmark VMS of menopause, were ranked over 3.5 on the bothersome scale in both Europe and the USA. Women in Europe experienced an average of 4.6 episodes of hot flushes/flashes and/or night sweats per day compared with 3.8 episodes per day in the USA.4
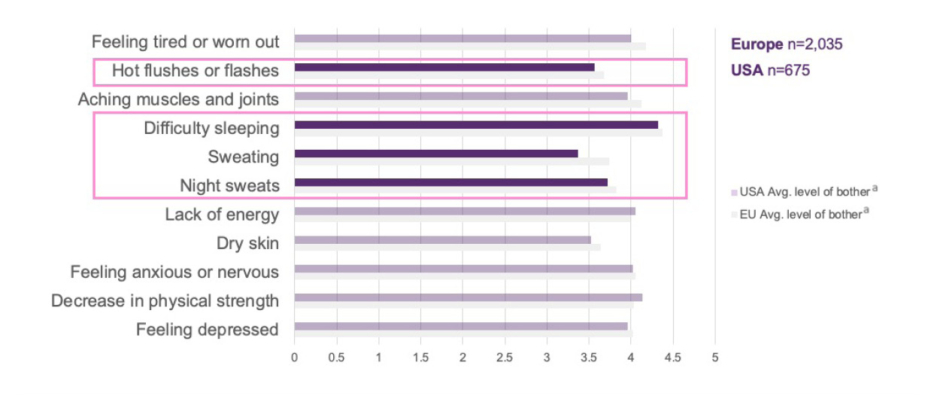
Figure 1: International survey of menopause symptoms and associated level of bother.1,4
ᵃRanked from 0 (not bothersome) to 6 (extremely bothersome), ≥4 is highly bothersome.
Note that the actual base varies per symptom.
Only selected symptoms are shown above. Dark purple bars denote VMS and sleep-related symptoms in the USA population.
Adapted from Nappi et al.4
Avg: average.
As Nappi outlined, the prevalence of VMS associated with menopause is influenced by many factors. These include psychological symptoms, smoking, diet, and BMI. VMS can also be impacted by external factors such as climate and the cultural context in which the woman lives.1,5-16
In addition to VMS, sleep disturbances are experienced by many women during menopause. Sleep disturbances are often associated with VMS but can be unrelated. Estimates indicate that between 40–60% of women suffer from disturbed sleep during the menopausal transition.17,18 Nappi stressed the importance of addressing sleep disturbances in midlife women due to their negative impact on physical and mental health, and quality of life.19 Sleep health is also recognised as one of the eight key pillars of cardiovascular (CV) health.20 During menopause, sleep disturbances are particularly associated with an increased number of nighttime awakenings and wakefulness after sleep onset, causing more sleep fragmentation.21,22 The prevalence of these menopause-related sleep issues appears to be broadly similar across different countries and ethnicities.4
In order to better help patients, healthcare professionals need to understand the interconnected symptom burden during the menopausal transition, Nappi explained (Figure 2).1 VMS, mood alterations, sleep disturbances, anxiety, and cognitive symptoms can frequently overlap.1,23,24 Menopause symptoms also have a direct effect on women’s daily lives, impacting them socially, economically, and functionally.2,25,26 The best way to address this symptomatology is therefore using a biopsychosocial model, Nappi suggested.1
Figure 2: The interconnected symptom burden during the menopausal transition.1,23
VMS: vasomotor symptoms.
Menopause Counselling
A major goal of the Women’s Health Academy is to empower women to actively participate in the management of their own menopause care.1,27 This is particularly important as menopause can mark a critical period in a series of risk factors related to cardiometabolic, vascular, musculoskeletal, and mental health, Nappi elaborated.1 Empowering women to participate and make decisions about their own menopause management requires healthcare professionals to provide access to realistic and balanced information, and challenge misconceptions around menopause related to stigma and gender-based ageism.1,27
As part of the empowerment process, Nappi stressed that it is important for healthcare professionals to recognise that many women will require help to address their menopause-related symptoms. Access to a supportive, well-informed clinician willing to listen and provide treatment as needed is therefore key. Decisions around menopause treatment should be made as part of a well-balanced and shared decision-making process. Setting realistic expectations from treatment is also crucial, Nappi pointed out.1
To facilitate women-centric menopause counselling in clinical practice, Nappi proposed a series of key principles for healthcare professionals to consider. Firstly, it is important to recognise the heterogeneous presentation of menopause symptoms. For the individual patient, the priority is to identify the most disruptive symptoms that require immediate attention. Healthcare professionals should provide personalised, evidence-based counselling, and consider whether any symptoms may have a more serious underlying cause. As part of this process, it is also important to offer tailored support strategies and personalised conversations, considering the women’s specific needs and preferences.1
Ultimately, the goal should be to facilitate women-focused menopause counselling through three key steps, Nappi summarised (Figure 3).1 Firstly, identify the most disruptive symptoms and the biggest health concerns. Secondly, focus on symptom relief using the most effective options for those symptoms and concerns. Thirdly, tailor the approach based on the patient’s preferences and nuances from their own medical history to achieve symptom relief and treatment adherence.1
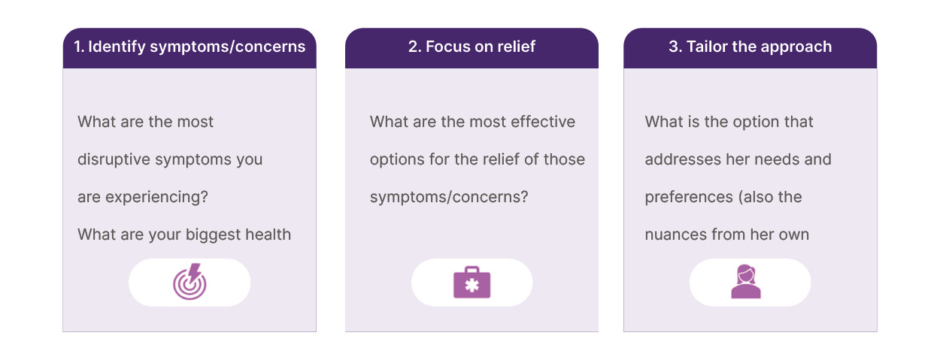
To illustrate the application of this 3-step menopause counselling model in clinical practice, experts presented and discussed a series of fictional case studies.1 “This approach is quite simple but it is novel, designed to help you as the clinician and your patient,” Jacobson explained.1
These are fictitious cases and proposed outcomes are based on clinician experience only. Individual cases may vary.
Case Study 1: Postmenopausal Woman with Genitourinary Syndrome of Menopause and Sexual Dysfunction
Firstly, Nappi presented the case of the fictional patient Elizabeth, a 68-year-old postmenopausal White woman who had her last menstrual period 16 years ago.1 The patient is retired, has two children, is a non-smoker, and has a BMI of 27 kg/m2 with gynoid weight distribution. Medical history reveals no relevant underlying conditions or gynaecological history, although she has a history of recurrent urinary tract infections and has previously received menopause hormone therapy (MHT) for VMS.1
Nappi outlined the main symptoms experienced by this patient as being genitourinary symptoms, including stress incontinence, sexual dysfunction, and frequent urination at night. Genitourinary symptoms are responsible for daily discomfort (not only during periods of active urinary tract infection), including irritation and pain. Stress incontinence has led to feelings of embarrassment, and she has low mood due to sexual dysfunction. Frequent urination at night also contributes to her fragmented sleep. As Nappi explained, the concern with this patient is that her symptoms may worsen over time without treatment, leading to detrimental effects on her long-term psychological wellbeing and quality of life. The patient herself has expressed a desire to seek therapy and is open to all eligible treatment options.1
The expert panel discussed the application of the 3-step counselling model to this patient. For Step 1, experts emphasised the importance of deciphering the highest priority symptom from the ‘laundry list’ of menopause-associated symptoms that women often present with. Given the limited consultation time allocated to each patient, Jacobson suggested that these questions could be posed to women in advance if possible, for example, through questionnaires/surveys or in nurse-led consultations. “Preparation in advance can lead to a more fulsome and productive consultation,” she advised. For this particular patient, the panel agreed that genitourinary syndrome of menopause symptoms, and associated low mood and sleep disturbances, appeared to be having the greatest impact on quality of life.1 “Once we know what is bothering the patient, we don’t need to discuss every treatment option for menopause but focus on treatment that is going to improve her symptoms,” Jacobson asserted. In Step 2 for this patient, Nappi indicated that for genitourinary syndrome of menopause symptoms she would recommend pelvic floor exercises, alongside other treatment options as appropriate (Nappi, personal communications).1,28
Step 3 involves tailoring treatment to each individual woman. For example, Nappi suggested that, in her experience, if the patient had comorbid rheumatoid arthritis and lacked dexterity, then oral MHT therapy may be preferrable to topicals.1 “These nuances can guide treatment,” Nappi advised (Nappi, personal communications).1
Case Study 2: Perimenopausal Woman with VMS and Sleep Disturbances Impacting Mood
The second fictional case study presented by Soares was Carol, a 45-year-old perimenopausal Black woman.1 She had made an appointment with her primary care physician after experiencing severe VMS, sleep disturbances, and mood changes over the past year. The patient works full time and has two children, aged 11 years and 13 years. Her last menstrual period was 6 months ago and she has no underlying relevant conditions or gynaecological history. She is a non-smoker with a BMI of 33 kg/m2 and an android weight distribution.1
In terms of symptoms and their impact, the patient is experiencing sleep disturbances 3–4 times per week, and severe VMS 5–6 times per week. The specific number of hot flashes per day is irrelevant here, Soares explained, if the patient is reporting that she is significantly bothered by them. During the transition to menopause, it is important to “respect patients’ wisdom to know what is affecting their quality of life more than we do,” Soares stressed. The hot flashes during the day are causing embarrassment and discomfort at work, and interrupted sleep at night. In turn, interrupted sleep is impacting the patient’s ability to work and complete simple day-to-day tasks and is lowering mood. Together, these symptoms are impacting her long-term psychological wellbeing and quality of life, compromising relationships and work performance.1
Again, the panel reiterated the importance of asking the right questions to ensure that the most disruptive symptoms associated with menopause are not missed. For this case study, the panel observed that the main bothersome symptom appears to be VMS. Hot flashes are in turn having a detrimental effect on the patient’s sleep. Soares confirmed that further tests may be required in some instances to explore other potential causes, but advice on sleep hygiene and treatment options to relieve VMS should still be offered as a key first step. For example, sleep apnoea affects approximately 35% of pre-menopausal women, impacting sleep.29 It is the job of the healthcare professional to explore this and other potential comorbid conditions, Soares reiterated.1
As this patient is receptive to therapeutic options, the panel agreed that treatment should focus on the relief of VMS, which have been identified as the most impactful symptom. In response to an audience question, Soares advised against simply prescribing magnesium for this patient due to insufficient evidence for its role as a sleep aid.30 Rather, he highlighted that the primary goal of treatment should be to minimise VMS, as this was indicated by the patient as the most bothersome symptom.1
Case Study 3: Postmenopausal Woman Recovering from Breast Cancer
Finally, Jacobson presented the fictional case of Helen, a 52-year-old Asian woman recovering from breast cancer and receiving ongoing treatment with tamoxifen.1 She has been menopausal for 1 year (unrelated to breast cancer treatment), has no known gynaecologic conditions or cardiovascular disease risk factors (gynoid weight distribution and BMI of 18.5 kg/m2), but has a family history of breast cancer. The patient works part time, has one adult child, and is a non-smoker. She has sought help from her primary care physician after struggling with VMS, characterised by daily hot flashes and sleep disturbances.1
Cancer survivorship is a complicating factor in this case, Jacobson stressed, and it is important to know the full details of the patient’s breast cancer history and their risk tolerance in order to recommend appropriate treatment. To this end, a detailed breast cancer history should be taken during the appointment. In particular, it is important to establish the chronology and timing from diagnosis, as women’s attitudes to survivorship may change over time. For many women who have recently undergone treatment for breast cancer, their key priority is to avoid any interventions that will increase the risk of recurrence, Jacobson emphasised. Understanding recurrence risk is therefore vital in order to make suitable menopause treatment recommendations. Jacobson highlighted features of the breast tumour that are important in this regard, such as stage (including size of tumour and presence of negative or positive axillary nodes); oestrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) status; oncotype score (if applicable); and results of any multigene panel tests. She stressed that establishing the type of breast cancer treatment the patient received and the duration of any ongoing treatment is also vital to direct suitable care for menopause symptoms (Jacobson, personal communications).1
Most importantly for Step 1 of this post-cancer menopause consultation, we need to know what symptoms the patient is having and which of these are impacting her most, Jacobson reiterated. In this case, the patient is experiencing menopause symptoms, including severe VMS and sleep disturbances (4–5 times per week), as well as anxiety and fear over breast cancer recurrence. She feels exhausted and irritable after daily VMS and frequent awakenings at night. These menopause symptoms are also contributing to worsening anxiety and fear over recurrence of breast cancer, which may impact the patient’s long-term psychological wellbeing and quality of life.1
Steps 2 and 3 of the menopause counselling model are paramount in this case, Jacobson explained, as the patient wants treatment to relieve her symptoms and is turning to her physician for advice on what is acceptable. The priority for the patient is concern about breast cancer recurrence, so we must take this into consideration, Jacobson advised, and use this to guide the treatment conversation. In this case, systemic MHT is unlikely to be a suitable treatment pathway due to its potential association with an increased risk of breast cancer recurrence, particularly in women with hormone receptor-positive disease.31 The fact that the patient’s symptoms began after starting tamoxifen therapy suggests that VMS may be due to its anti-oestrogen effects rather than pre-existing VMS prior to breast cancer diagnosis, Jacobson explained (Jacobson, personal communications).1,32
Overall, the panel agreed that in a patient like this with specific contraindications or considerations around MHT, it is important to tailor the approach and focus on the most bothersome symptom to gain maximum quality-of-life improvement. By starting with treatment for the most impactful symptoms, in this case VMS, it may be possible to improve many of the symptoms that are “downstream on the patient’s list,” Jacobson advised. Panel members pointed out that patients who have had cancer often think that adverse events associated with breast cancer treatment must be accepted in order reduce cancer recurrence risk. It is therefore important to explain that options are available to treat menopause symptoms in these cohorts of patients.1
Summary
Menopause is a highly individual experience that requires tailored solutions. Treatment approaches should therefore be personalised and guided by a woman’s symptoms, risk profile, health history, and personal preferences, rather than by recommendations applied uniformly to all women. A 3-step approach to menopause counselling should be adopted to identify both the physical and psychological symptoms of menopause, respecting the diversity of the woman’s experiences and needs. Step 1 is to identify the most disruptive symptoms and biggest health concerns, Step 2 is to focus on effective options for symptom relief, and Step 3 is to tailor the approach to the patient’s individual needs and preferences.1
It is important to individualise treatment, as there is no ‘one-size-fits-all’ approach for menopause care, Soares reiterated. The 3-step model is designed to enable clinicians “to efficiently and humanly tailor your menopause consultation and treatment approach to the patient who is in front of you,” he concluded.1
This symposium was highly participative, encouraging attendees to rethink the way they usually approach menopause care and inviting them to listen to their patients and prioritise their concerns. Importantly, it also fostered frank discussions among experts from various disciplines in pursuit of more comprehensive, patient-centred care.1
MA-PFM-WHC-ALL-0071-1 | MA-PFM-WHC-GB-0006 | June 2026






