BACKGROUND AND AIMS
In a collaborative analysis of lipid-lowering therapy trials, high-sensitivity C-reactive protein (hsCRP) was a stronger predictor of cardiovascular risk than low-density lipoprotein cholesterol.1 Most participants in these trials had diabetes (76%), a condition associated with elevated inflammatory markers including hsCRP, IL-6, and IL-18, which predict cardiovascular outcomes.2-5 More complex coronary artery disease (CAD) in diabetes is also associated with adverse cardiovascular outcomes, whereas in non-complex disease, outcomes are similar to patients without diabetes.6
Therefore, the authors aimed to explore the relationship between inflammation, defined by established blood biomarkers, and CAD extent in Type 2 diabetes (T2D).7
MATERIALS AND METHODS
This was a single-centre study prospectively recruiting patients presenting with acute coronary syndrome. hsCRP was performed clinically upon presentation. Plasma was isolated at follow-up. hsCRP, IL-6, and IL-18 were measured using the Ella apparatus (ProteinSimple™ [Bio-Techne, Minneapolis, Minnesota, USA]) as per manufacturer. Invasive coronary angiography was analysed then scored using Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery (SYNTAX), blinded to diabetes status and biomarkers. CAD extent was dichotomised to high versus low SYNTAX using clinically established cut-offs (high >22, low ≤22).
Statistical analyses used t-test/analysis of variance or the Mann–Witney/Kruskal–Wallis test as appropriate, and multivariable linear regression was performed.
RESULTS
One hundred and sixteen participants consented to the study; 62 (53.4%) had T2D or pre-diabetes. The mean (±SD) age was 66±10.2 years. Ninety-nine participants had hsCRP measured clinically at median 0 (interquartile range: 0–1) days from admission. Plasma was isolated at follow-up, median 57 (44–72) days from discharge in 86 participants. CAD extent, defined by SYNTAX score, was similar between patients with and without T2D or pre-diabetes (mean: 24±11.9 versus 22±11.9; p=0.513). At admission, patients with T2D or pre-diabetes had higher hsCRP (median: 3.90 [1.4–8.0] versus 2.35 [1.1–4.4] mg/L; p=0.09).
When participants were dichotomised by CAD extent, hsCRP was significantly higher in patients with high SYNTAX scores (3.9 [1.6–8.7] versus 1.9 [1.0–4.5] mg/L; p=0.01) (Figure 1A) but more so in diabetes (5.1 [2.6–11.0] versus 2.5 [1.6-5.8] mg/L; p=0.052) (Figure 1B). Adjusting for age, sex, and BMI using multivariate linear regression, high SYNTAX score (β=0.32; p=0.002) and diabetes (β=0.25; p=0.01) were independently associated with higher hsCRP.
At follow-up, hsCRP was similar between participants with and without diabetes (median: 1.5 [0.9–3.6] versus 1.2 [0.5–5.0] mg/L; p=0.223). After adjustment for age, sex, BMI, and patients who had coronary artery bypass grafting, the association with hsCRP, CAD extent, and diabetes status, which was demonstrated at admission, was lost.
IL-6 and IL-18 were higher in patients with T2D or pre-diabetes (median: 4.64 [2.80–6.35] versus 3.38 [2.03–4.76] pg/mL; p=0.051 and 340 [266–422] versus 274 [224–369] pg/mL; p=0.032, respectively). After adjusting for covariates, diabetes was independently associated with IL-18 (β=0.08; p=0.044), but there was no association between IL-6 and IL-18 with CAD extent.
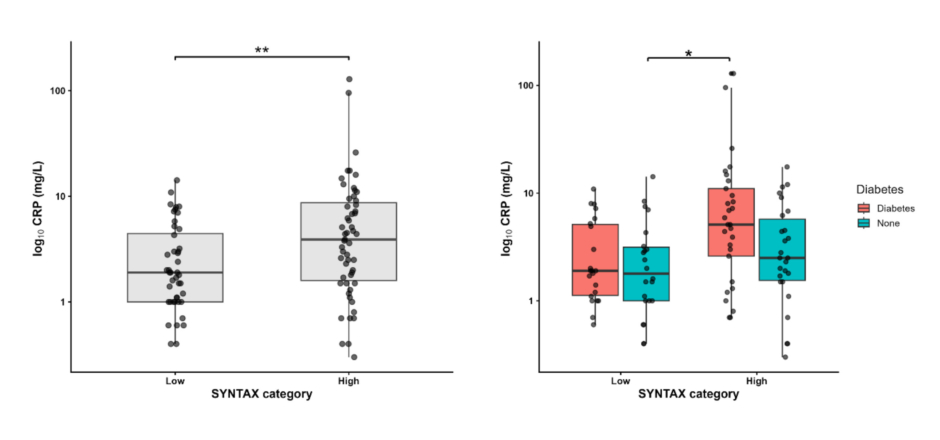
Figure 1: Relationship between hsCRP and SYNTAX score (A) stratified by diabetes status (B).
* p value < 0.05
** p value < 0.01
CRP: C-reactive protein; hsCRP: high-sensitivity C-reactive protein; SYNTAX: Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery.
CONCLUSION
The authors demonstrated that C-reactive protein (CRP) upon presentation with acute coronary syndrome, but not at follow-up, was associated significantly with extensive CAD and diabetes. Measurement of CRP during the acute presentation of CAD is often systematically excluded, and is primarily focused on the rehabilitation or baseline period. However, this study suggests that elevation of hsCRP acutely may identify a propensity to inflammation that is relevant to CAD.





