Abstract
Pleural tuberculosis is a common extrapulmonary manifestation of Mycobacterium tuberculosis, presenting with non-specific respiratory and constitutional symptoms. Diagnostic confirmation is often difficult due to the paucibacillary nature of pleural fluid. However, molecular tools such as the GeneXpert MTB/RIF assay (Cepheid, Sunnyvale, California, USA) have improved microbiological diagnosis. The authors present a case of pleural tuberculosis in a 37-year-old Nigerian male with microbiological confirmation and a review of diagnostic strategies.
Key Points
1. Pleural tuberculosis can occur with negative sputum studies, complicating early diagnosis.2. GeneXpert MTB/RIF assay (Cepheid, Sunnyvale, California, USA) on pleural fluid enabled microbiological confirmation in this case. Elevated pleural fluid adenosine deaminase and lactate dehydrogenase also supported the diagnosis in the absence of culture growth.
3. The integration of clinical, biochemical, and molecular tools improves diagnostic accuracy in resource-limited settings like Nigeria.
INTRODUCTION
Tuberculosis remains a major public health issue globally, particularly in low- and middle-income countries. Nigeria ranks among the top 10 countries with the highest tuberculosis burden according to the WHO.1 Extrapulmonary tuberculosis accounts for up to 20% of cases in immunocompetent individuals, with pleural tuberculosis being the most common form.Pleural tuberculosis often presents with unilateral exudative pleural effusion, chest pain, fever, and weight loss. Diagnosing pleural tuberculosis remains a challenge due to the low bacillary load in pleural fluid. Traditional diagnostic modalities like Ziehl–Neelsen staining and culture often yield poor sensitivity. Biochemical markers such as elevated adenosine deaminase (ADA) and lactate dehydrogenase (LDH) are supportive, while nucleic acid amplification tests like GeneXpert MTB/RIF (Cepheid, Sunnyvale, California, USA) have improved sensitivity and specificity for pleural tuberculosis.2-5
This report is informative, as it elucidates the need for a high index of suspicion, as well as corroboration of clinical findings and molecular testing, especially in the background of atypical pleural findings and negative sputum studies in resource-limited and tuberculosis endemic environments.
CASE PRESENTATION
A 37-year-old male truck driver presented with a 3-week history of dry cough, which later became productive of whitish, non-foul-smelling sputum. He reported associated high-grade intermittent fever, chills, rigors, pleuritic chest pain, weight loss, and night sweats. He had no history of contact with individuals with chronic cough, smoking, and exposure to biomass fuel, occupational dust, or poultry. No recent travel or unpasteurised milk intake was reported.
Physical examination revealed a patient who was alert and not in respiratory distress, afebrile, not pale, anicteric, and without finger clubbing, lymphadenopathy, or pedal oedema. Respiratory exam showed a respiratory rate of 20 cycles per minute, and oxygen saturation level was 95% on room air, with reduced chest expansion on the right, central trachea, dull percussion note, reduced tactile fremitus and vocal resonance, and diminished breath sounds in the right mid and lower lung zones. Cardiovascular examination revealed a pulse rate of 75 bpm, blood pressure of 137/84 mmHg, and first and second heart sounds with no murmur. Abdominal examination was unremarkable.
INVESTIGATIONS
Initial laboratory investigations were done, revealing a markedly elevated erythrocyte sedimentation rate of 110 mL/hour, indicative of an inflammatory condition. Other haematological and biochemical parameters were within normal range. Microbiological screening for HIV I and II serology was negative. Sputum evaluation, including acid fast bacilli microscopy and GeneXpert MTB/RIF assay, did not detect Mycobacterium tuberculosis. Sputum gram staining and bacteriologic culture showed no bacterial growth (Table 1[/hl).
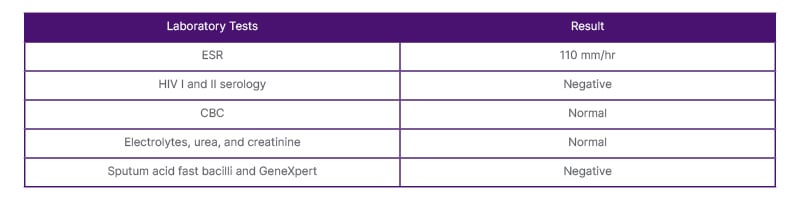
Table 1: Baseline laboratory investigations of the patient.
CBC: complete blood count; ESR: erythrocyte sedimentation rate; GeneXpert: Cepheid, Sunnyvale, California, USA.
A plain chest radiograph showed right-sided pleural effusion with a meniscus sign. Chest CT revealed massive right-sided pleural effusion with underlying consolidation, ground-glass opacities, and linear densities suggestive of atelectasis or fibrosis (Figure 1).
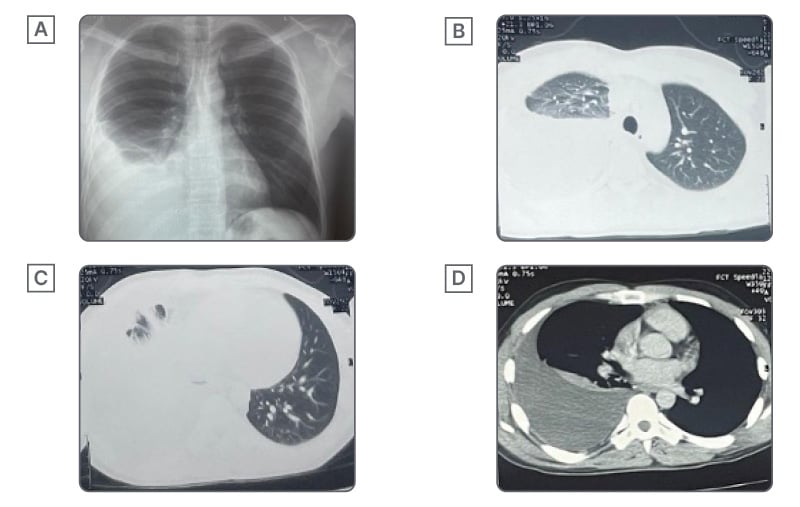
Figure 1: Radiological features of right-sided pleural tuberculosis demonstrating massive pleural effusion with associated parenchymal changes on chest radiograph and CT.
A) X-ray before thoracocentesis. B, C) CT scan of the upper and lower lobe of the lung window. D) Axial view of mediastinal window.
A diagnostic thoracocentesis was performed through an aseptic procedure, which yielded amber, cloudy pleural fluid. Pleural fluid analysis revealed features of exudative effusion with elevated ADA and LDH, and reduced glucose concentration. Elevated ADA is supportive of tuberculous cause, in corroboration with other findings. Cytological assessment showed an atypical feature of an absent white blood cell, which is unusual in pleural tuberculosis.
The pleural fluid gram staining and culture showed no bacterial growth; however, pleural fluid GeneXpert MTB/RIF detected M. tuberculosis (Table 2).
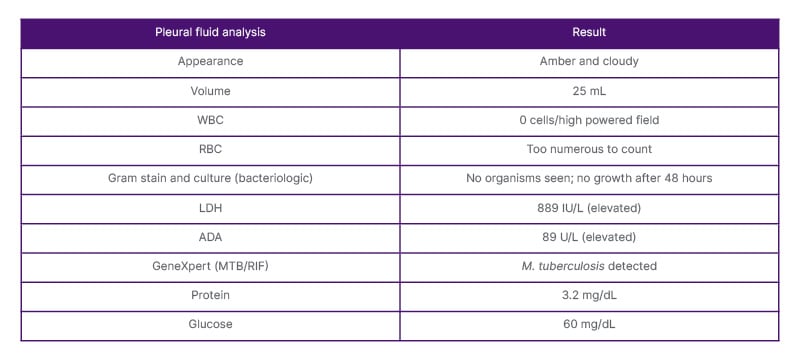
Table 2: Pleural fluid biochemical, cytological, and microbiological analysis.
ADA: adenosine deaminase; GeneXpert: Cepheid, Sunnyvale, California, USA; LDH: lactate dehydrogenase; RBC: red blood cells; WBC: white blood cells.
DIAGNOSIS
The diagnosis of pleural tuberculosis was made based primarily on the microbiological detection of M. tuberculosis in pleural fluid via GeneXpert, supported by elevated ADA and LDH levels and the presence of a unilateral exudative pleural effusion in a symptomatic patient.
MANAGEMENT
The patient was commenced on standard anti-tuberculous therapy with a 2 month intensive phase of a daily dose of isoniazid 300 mg, rifampicin 600 mg, pyrazinamide 1,600 mg, and ethambutol 550 mg, followed by 4 months of continuation phase with a daily dose of isoniazid 300 mg and rifampicin 600 mg. Therapeutic thoracentesis was performed to relieve respiratory symptoms. The patient received adherence counselling and supportive care.
OUTCOME AND FOLLOW-UP
At 1-month follow-up, the patient showed significant clinical improvement, including resolution of fever and night sweats, weight gain, and reduced chest discomfort. He remained adherent to medications. He completed a course of anti-Koch, repeat chest radiograph showed resolution of pleural effusion, and erythrocyte sedimentation rate became normal.
DISCUSSION
Pleural tuberculosis is the second most common extrapulmonary tuberculosis,6 with a prevalence of 30% in tuberculosis endemic areas. Diagnosis is challenging, owing to its paucibacillary nature and non-specific clinical characteristics.7 This case report highlights the multimodal diagnostic approach to a middle-aged Nigerian man with pleural tuberculosis in a high-burden area and resource-limited setting.
Pleural tuberculosis is due to an immune-mediated response to the rupture of subpleural parenchymal focus into the pleural cavity.8 Typical clinical presentation is exudative unilateral pleural effusion, usually right-sided, alongside pleuritic chest pain, cough, and fever.7 Pleural fluid finding in tuberculosis commonly has an appearance of a straw-coloured exudate characterised by lymphocytic predominance on cytology, elevated pleural protein, high LDH, and reduced glucose in contrast to serum glucose.9 Pleural fluid biomarkers also have an important role in diagnosis, especially in resource-limited settings.
ADA, one of the commonly used pleural fluid biomarkers, has high positive predictive value in high-burden areas, with a Nigerian study reporting its presence in 85% of patients with pleural tuberculosis.10 A meta-analysis that analysed ADA at a cut-off of 40±4 IU/L, revealed a pooled sensitivity and specificity at 93% and 90%, respectively.11 Pleural ADA is not totally specific, considering that it could be confounded by rheumatological conditions and cancers.8 Pleural interferon gamma is another useful biomarker, and a meta-analysis demonstrated its superiority to ADA.12 However, ADA, which is cost effective, is a valuable diagnostic tool in resource-limited settings when analysed in combination with radiographic, mycobacteriologic, and clinical features.13 Novel biomarkers such as pleural fluid soluble fluid IL-2 receptor, lysozyme, IL-27, interferon gamma release assay, and Aptamer-Linked Immobilized Sorbent Assay (ALISA) have also been studied, with their varying sensitivity and specificity.9,14,15 Owing to its low bacillary load and associated diagnostic challenges, this has led to emerging evidence showing that transcriptional pleural fluid signatures, such as caspase recruitment domain family member 17 (CARD17), guanylate binding protein 2 (GBP2), and complement C1q subcomponent subunit B (C1QB), and potential proteomic biomarkers, such as LV218, have excellent profiles.16,17 However, most of these potential biomarkers were studied in the non-African population, thereby needing further validation in resource-limited settings such as the sub-Saharan African population.
The paucibacillary nature of pleural tuberculosis makes microbiological confirmation with mycobacterial culture and Zhiel–Neelsen staining difficult. Thoracoscopic-assisted pleural biopsy revealing granulomatous inflammation is considered the gold standard.3,9 However, in resource-constrained settings where funding might be an issue, the deployment of nucleic acid amplification tests such as GeneXpert RIF/MTB is of benefit.
Although having modest sensitivity and high specificity, as demonstrated in a meta-analysis, its use aligns with global recommendations such as the WHO.5
Pleural fluid findings of elevated protein, LDH, and detection of M. tuberculosis through GeneXpert MTB/RIF in the authors’ patient is consistent with studies.4,9 In contrast to several pieces of evidence showing lymphocytic predominance in pleural tuberculosis,4,9 the unusual absence of pleural white blood cells in this patient might be explained by a possible cytological assessment method in a high powered field, rather than the standard automated nucleated cell count with differentials. Arrigo et al.18 reported an advantage of automated nucleated cell count over manual methods of counting. However, his clinical presentation, with pleural fluid biochemical findings, and detection of Mycobacterium with high-specificity GeneXpert MTB/RIF support the diagnosis of pleural tuberculosis.
Follow-up revealed an improved response of the authors’ patient to the standard 6-month antitubercular therapy (2 months of isoniazid, rifampicin, pyrazinamide, and ethambutol followed by 4 months of isoniazid and rifampicin), as espoused in current recommendations.19 This further reinforces the possibility of the authors’ diagnosis and the need for timely intervention, even with limited investigation accessible in resource-limited settings and endemic areas.
The absence of a full biochemical profile, histological confirmation, and low sensitivity of nucleic acid testing is a limitation in these findings. However, this case emphasises the importance of a corroborating clinical assessment alongside modalities of pleural fluid analysis, biomarkers, and microbiological confirmation in diagnostic approaches in endemic areas with resource limitation. It demonstrates that the microbiological confirmation through GeneXpert and other modalities amidst atypical pleural fluid finding could help to prevent delayed diagnosis.
CONCLUSION
Pleural tuberculosis should be considered in patients with unilateral pleural effusion and constitutional symptoms, especially in endemic regions.
GeneXpert MTB/RIF and ADA analysis are valuable tools that enable early and accurate diagnosis, even in sputum-negative cases. Timely microbiological confirmation facilitates prompt treatment initiation and improved outcomes.




