BACKGROUND AND AIMS
Paget’s disease of bone (PDB) is a focal, benign disorder of bone metabolism first described by Sir James Paget in 1876. It affects approximately 1% of the general population.1 Uncomplicated Paget’s disease is generally diagnosed in individuals aged 55 years or older and shows a slight male predominance. The associated morbidity varies depending on the site and number of lesions. The main clinical manifestations are bone pain, deformities in affected areas, and a heightened risk of fracture, although many patients remain asymptomatic.2,3 There has long been an association between Paget’s disease and an increased risk of osteosarcoma, usually occurring in individuals with long-standing, polyostotic disease and typically affecting patients in their seventh decade of life.4 While PDB lesions predominate in the axial skeleton, skull, femurs, and tibias, Pagetic osteosarcomas are more commonly found in the pelvis, femur, humerus, and skull. This is somewhat different from osteosarcoma in adolescents, which shows a predilection for the femur. The reason for this discrepancy remains unknown. Osteosarcomas are rare cancers, predominantly occurring in adolescents and young adults during their second and third decades of life, and account for approximately 5% of childhood cancers.5 The incidence of malignancies, including sarcomas related to Paget’s disease, has been documented across numerous studies, emphasising its complex nature in certain geographic populations and suggesting varied outcomes.6
CASE PRESENTATION
A 55-year-old female presented with a sudden onset of pain in the left arm and right hip. An X-ray of the left arm (Figure 1) revealed a pathological fracture and bone tumour in the left distal humerus. A pelvic X-ray (Figure 2) showed PDB in both femoral heads. A whole-body bone scan (Figure 3) revealed images indicative of PDB in the skull, left humerus, fourth lumbar vertebra, and pelvic bones. Laboratory investigation demonstrated an elevated alkaline phosphatase (ALP) level of 671 U/L (normal range: 30–105 U/L). Biopsy samples taken from the tumour in the left humerus confirmed a high-grade osteoblastic osteosarcoma.
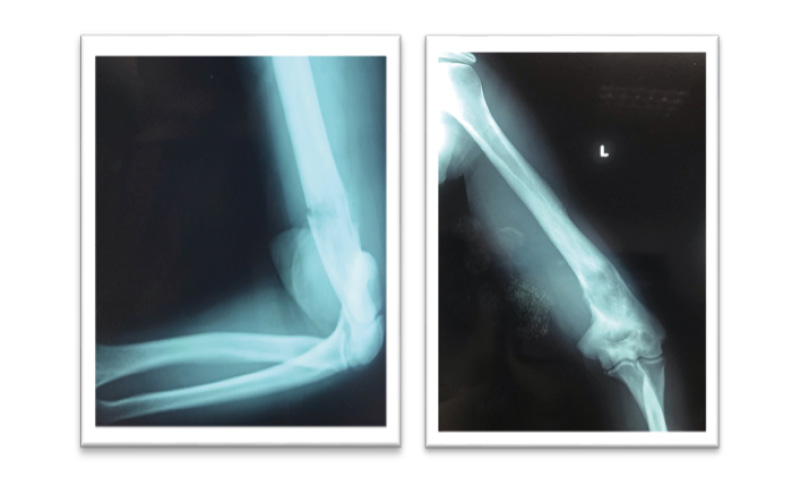
Figure 1: X-ray of the left arm showing a pathological fracture and bone tumour in the distal humerus (A-P, L-L).
A-P: anterior-posterior; L-L: latero-lateral.

Figure 2: A-P pelvis X-ray demonstrating Paget’s disease of both femoral heads.
A-P: anterior-posterior.
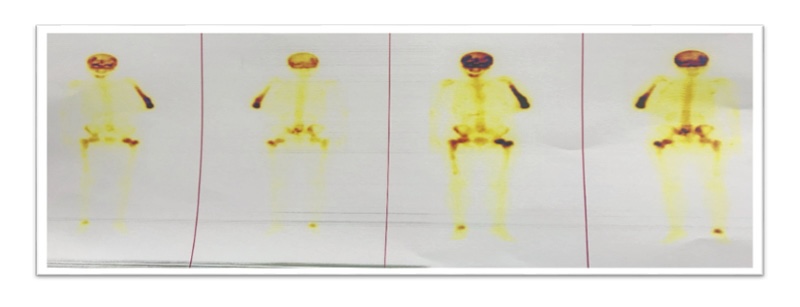
Figure 3: Radionuclide whole-body bone scan indicating PDB images in the skull, left humerus, fourth lumbar
vertebra, pelvic bones, and right talocrural joint.
PDB: Paget’s disease of bone.
CASE PRESENTATION
A 55-year-old female presented with a sudden onset of pain in the left arm and right hip. An X-ray of the left arm (Figure 1) revealed a pathological fracture and bone tumour in the left distal humerus. A pelvic X-ray (Figure 2) showed PDB in both femoral heads. A whole-body bone scan (Figure 3) revealed images indicative of PDB in the skull, left humerus, fourth lumbar vertebra, and pelvic bones. Laboratory investigation demonstrated an elevated alkaline phosphatase (ALP) level of 671 U/L (normal range: 30–105 U/L). Biopsy samples taken from the tumour in the left humerus confirmed a high-grade osteoblastic osteosarcoma.
The patient commenced treatment with three doses of intravenous doxorubicin and cisplatin chemotherapy. Following the third dose, she received a single intravenous injection of 5 mg zoledronic acid for PDB. The chemotherapy was well tolerated without side effects, and the patient reported improvement in bone pain following the zoledronic acid infusion. The ALP level decreased to 153 U/L and normalised within 2 months. After three cycles of chemotherapy, MRI of the primary tumour and re-evaluation with the orthopaedic surgeon were conducted. While there was a good clinical response to chemotherapy, no significant reduction in tumour mass was observed. Due to the absence of an option for conservative surgery, amputation of the left arm was performed by the orthopaedic surgeon. After the amputation, the patient underwent three more cycles of chemotherapy with the same regimen, which she tolerated well. She is currently under surveillance from both her oncologist and rheumatologist.
DISCUSSION
PDB is often diagnosed through incidental findings in routine blood chemistry panels, particularly elevated ALP levels, or through imaging performed for unrelated reasons. In this case presentation,7 PDB was diagnosed through radiological investigation prompted by a humeral fracture caused by a bone tumour. The incidence of malignant transformation in PDB can reach 30% in older patients.8 Notably, the authors’ patient is younger than the typical age when osteosarcomas usually occur, which is often in the seventh decade of life.9 The proportion of osteosarcoma cases associated with PDB in individuals over 60 years may be as high as 50%.10 This aligns with findings in Paget’s sarcoma literature, which detail outcomes from various registries and studies highlighting the significance of timely diagnosis and management.6
CONCLUSION
This case highlights the rare but serious risk of osteosarcomatous transformation in PDB, even in a patient younger than the typical age for Pagetic sarcoma. Prompt recognition through imaging and biochemical markers (markedly elevated ALP) enabled timely biopsy and initiation of multimodal therapy. Although limb-sparing surgery was not achievable and amputation was required, systemic chemotherapy combined with a single zoledronic acid infusion resulted in clinical improvement and normalisation of ALP, and the patient remains under multidisciplinary surveillance. Clinicians should maintain a high index of suspicion for malignant change in patients with Paget’s disease who develop new localised pain, pathological fractures, or focal radiographic progression, and management should involve coordinated oncologic, orthopaedic, and metabolic bone disease expertise.






