Funding statement: The publication of this independently commissioned article was funded through a grant by LEO Pharma A/S, with no input on editorial content except for a check on factual accuracy.
Authors: Yolande Chalmers,1 Raj Chovatiya,2,3 Benjamin D. Ehst,4 Mark G. Kirchhof,5,6 Andrei Metelitsa,7,8 Andrew Pink,9,10 Simone Ribero,11 Diamant Thaçi12
1. European Medical Journal (EMJ), London, UK
2. Chicago Medical School, Rosalind Franklin University of Medicine and Science, North Chicago, USA
3. Center for Medical Dermatology + Immunology Research, Chicago, USA
4. Oregon Medical Research Center, Portland, USA
5. Division of Dermatology, Faculty of Medicine, University of Ottawa, Canada
6. The Ottawa Hospital, Canada
7. Division of Dermatology, University of Calgary, Canada
8. Beacon Dermatology, Calgary, Canada
9. St John’s Institute of Dermatology, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
10. King’s College London, UK
11. Dermatology Clinic, Department of Medical Sciences, University of Turin, Italy
12. Institute and Comprehensive Centre for Inflammation Medicine, University of Lübeck, Germany
Conflicts of interest: Chalmers has declared no conflicts of interest. Chovatiya has served as an advisor, consultant, speaker, and/or investigator for AbbVie, Acelyrin, Almirall, Alumis, Amgen, AnaptysBio, Apogee Therapeutics, Arcutis Biotherapeutics, Argenx, Astria Therapeutics, Avalere Health, Beiersdorf, BioCryst Pharmaceuticals, Boehringer Ingelheim, Bristol Myers Squibb, Cara Therapeutics, Castle Biosciences, Celldex Therapeutics, CLn Skin Care, Dermavant, DKSH, Eli Lilly and Company, EMD Serono, Enveda Therapeutics, EPI Health, Formation Bio, Forte Biosciences, Galderma, Genentech, GSK, Incyte, Imagene Bio, Immunocore, Indero, Johnson & Johnson, Kenvue, LEO Pharma, L’Oréal, Nektar Therapeutics, Nia Health, Novan, Novartis, Opsidio, Organon, Pfizer, Propeller Bio, RAPT Therapeutics, Regeneron, Sanofi, Sitryx, SUN Pharma, Takeda, TRex Bio, UCB, Zai Lab, ZenZema, and Zuellig Pharma. Ehst has served as an advisory board member, consultant, contributor, speaker, and/or investigator for AbbVie, Aclaris Therapeutics, Allakos, Almirall, Alumis, Amgen, Arcutis Biotherapeutics, BMS, Celldex, Celgene, Concert Phramaceuticals, Dermavant Sciences, DermBiont, Eli Lilly, Evelo Biosciences, Evommune, Incyte, Janssen Biotech, Kymab, LEO Pharma, National Psoriasis Foundation, Navigator Medicines, Novan, Novartis, Ortho Dermatologics, Priovant, Pfizer, Regeneron, Sanofi-Genzyme, Takeda, UCB, Up-To-Date, and Ventyx Biosciences. Kirchhof has served as a speaker and/or advisor/consultant for, and has received grants, honoraria, or consulting fees from, AbbVie, Amgen, Arcutis, Bausch Health, BioJamp, Boehringer Ingelheim, Eli Lilly, Incyte, Johnson & Johnson, LEO Pharma, Novartis, Organon, Pfizer, Recordati, Sanofi-Aventis, Therakos, and UCB; serves as president and member of the board for the Canadian Dermatology Association; and is a member of the board for the National Capital Skin Diseases Foundation. Metelitsa has served as a speaker and researcher for AbbVie, Amgen, Apogee, Arcutis, Bausch, BMS, Eli Lilly, Galderma, Incyte, Janssen, Leo, Pfizer, Organon, Sanofi, Sun Pharma, and UCB. Pink has acted as an investigator, speaker, advisor, and received educational support and/or research funding from Sanofi, Leo, Almirall, Galderma, Amgen, Pfizer, Lilly, Abbvie, Novartis, J&J, BI, UCB, BMS, Incyte, and Celgene. Ribero has received research grants/travel support/consultancy fees from AbbVie, Almirall, Leo Pharma, J&J, L’Oréal, Sanofi Regeneron, Sandoz, UCB, Eli Lilly, Novartis, BMS, and Incyte. Thaçi has served as an investigator and/or consultant/advisor for AbbVie, Almirall, Amgen, BMS, Boehringer Ingelheim, Celltrion, Eli Lilly, Galderma, Incyte, Johnson & Johnson, Kyowa Kirin, LEO Pharma, L’Oréal, New Bridge, Novartis, Pfizer, Regeneron, Samsung, Sanofi, Stada, Takeda, Target-RWE, UCB, Viatris, and Vichy; and received grants from AbbVie, Almirall, LEO Pharma, Novartis, and UCB.
Acknowledgements: Medical writing and discussion moderation were provided by Yolande Chalmers, EMJ, London, UK.
Received: 12.03.26
Accepted: 18.04.26
Keywords:Atopic dermatitis (AD), burden, difficult-to-treat, face, feet, hands, head and neck, high-burden areas, systemic therapy.
Citation: EMJ. 2026;11[2]:95-106. https://doi.org/10.33590/emj/W0N7I9MC
Abstract
Atopic dermatitis (AD) involving sensitive and/or visible hard-to-treat areas, including the head and neck, face, hands, feet, and genital regions, is associated with a significant psychosocial and clinical burden. AD involving these high-burden areas is commonly associated with diminished patient quality of life and a range of management challenges for patients and clinicians. There is a notable lack of epidemiological evidence investigating these regions, with experts highlighting that high-burden areas are poorly defined and under-studied. Evidence to inform clinical practice often comes from sub-analyses, and there is a clear need for more directed research into optimal treatment of high-burden regions.
Advancing knowledge of AD pathophysiology has enabled a better understanding of the burden of disease and, along with it, a new generation of targeted therapies. Real-world evidence evaluating the safety and effectiveness of these systemic treatments is increasingly crucial for clinicians to understand and apply their impact when making decisions in routine clinical practice for patients with AD in high-burden areas.
A panel of seven expert dermatologists convened for a series of virtual roundtable discussions, conducted on 18th February, 27th February, and 5th March 2026. Experts discussed a series of questions in a roundtable discussion based on pre-read literature provided before the discussion, focusing on unmet needs in high-burden AD, and emerging clinical data on biologic treatment. Discussion was moderated by the medical writer. This article presents excerpts from the expert roundtable discussion on high-burden areas in AD, covering understanding high-burden AD and its associated challenges, the current treatment landscape, and ongoing unmet needs. In particular, the expert roundtable discussion highlighted a need for consistent terminology, clear clinical guidance, and robust data on systemic management specific to AD affecting high-burden areas. Patient disease burden, unmet needs, access to systemic treatments, and emerging data informing potential individualised AD management were explored.
Key Points
1. Atopic dermatitis in high burden areas (head and neck, face, hands, genitals, and feet) is associated with increased clinical severity and psychosocial and occupational burden, requiring comprehensive, multifaceted management.2. Management of moderate-to-severe high-burden atopic dermatitis is typically systemic, with treatment selection balancing symptom control, patient-reported quality of life, desired outcomes, adverse event risks, and broader healthcare considerations.
3. Experts highlighted emerging evidence on biologic therapies in high-burden areas, emphasising the importance of ongoing research to support tailored, site-specific treatment strategies and improved outcomes for patients.
UNDERSTANDING HIGH-BURDEN AREAS IN MODERATE-TO-SEVERE AD
What Constitutes a High-Burden Area?
Atopic dermatitis (AD) is a common, heterogeneous, and chronic relapsing inflammatory disease characterised by pruritus and eczematous, erythematous inflamed lesions, often across multiple body areas.1,2 The disease is characterised by variable onset, unpredictable flare-ups, and fluctuating severity, which contribute to difficulties in disease management.1,2 Involvement of high-burden, sensitive, and/or visible and functionally important areas, such as the head and neck, face, hands, genitals, and feet, is common and can substantially exacerbate both clinical and psychosocial burden.3,4 These regions can be particularly difficult to conceal, associated with an occupational burden, and impact quality of life (QoL), social interactions, self-esteem, and work productivity, providing clinical challenges for long-term management and disease control.4
The Substantial Real-World Impact of High-Burden AD
Real-world evidence reflects the significant impact of AD in high-burden areas. Data from the Danish Severe and Chronic Atopic Dermatitis Treatment CoHort (SCRATCH) Registry (N=282),5 a nationwide registry of adults with moderate-to-severe AD, demonstrated that patients with moderate-to-severe AD experience substantial impairment of QoL and work ability. Involvement of the head and neck was associated with worse QoL, with similar results reflected across USA and European studies,4,6 highlighting the increased impact of disease when occurring in these high-burden, sensitive areas.
In a 2020 USA Adelphi Disease Programme Survey (n=150 physicians; n=599 adult patients), real-world data from patients and physicians were collected to investigate the impact of lesion locations on patient QoL.4 Among surveyed patients with AD, all lesions affected QoL, but lesions present in visible areas had the most impact on patient QoL.
Areas with AD lesions assessed were head and neck, upper extremities, lower extremities, front, back, face, hands/fingers, feet/toes, and pelvis/genitals. Front included the pelvis, genitals, abdomen, and chest.4 The head and neck were considered the most bothersome (68%), alongside hands and fingers (58%), front (30%), and upper extremities (22%), all of which were reported as having statistically significant associations with Dermatology Life Quality Index (DLQI) items (Figure 1). Moreover, lesions located on the hands/fingers and head/neck were associated with increased impact on the anxiety and depression dimension of the EuroQoL 5-Dimension tool.4
Experts agreed that reported real-world evidence reflects their experience with patients in clinical practice. Patients with high-burden area involvement often experience a high burden of disease, with notable negative impact on patient QoL, as well as physical and psychosocial impacts. The unpredictable nature of flares, particularly in visible or intimate areas, can contribute to anxiety and depression around social interactions, whilst the involvement of hands and feet can impact a patient’s ability to work or perform daily activities. The management of high-burden areas, especially the face, can be challenging, as use of topical therapies can be limited and patients with face and neck involvement can show significantly greater disease involvement across the rest of the body.3-8
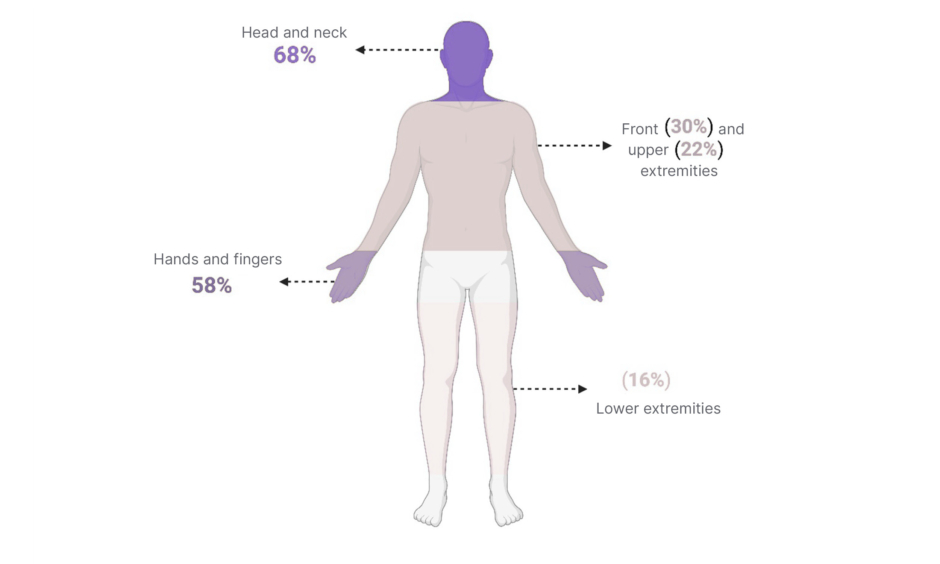
Figure 1: Most burdensome lesion locations reported by clinicians and patients with moderate-to-severe AD.4
In a USA survey (n=150 physicians; n=599 adult patients), data from patients and physicians were collected to investigate impact of lesion locations on patient QoL.
Adapted from Lio et al.4 Created in biorender.com.
AD: atopic dermatitis; QoL: quality of life.
SYSTEMIC THERAPY FOR MODERATE-TO-SEVERE AD IN HIGH-BURDEN AREAS
The prevention and management of AD typically begin with emollient restoration of the skin barrier, and, for acute flares, topical corticosteroids (TCS).7 For patients with mild-to-moderate AD, the disease can often be controlled with topical treatments. However, those with moderate-to-severe disease may require systemic therapy to achieve long-term disease control.7,9
Over the past decade, the emergence of targeted systemic therapies has revolutionised the treatment landscape of moderate-to-severe AD, with advanced therapies demonstrating durable efficacy and tolerable safety profiles in patients with moderate-to-severe AD.7,10 Biologic therapies act through the targeting and inhibition of AD-specific drivers like IL-13, IL-4, and IL-31, whilst small molecule JAK inhibitors block specific enzymes within the JAK-signal transducer and activator of transcription pathway.11 Conventional systemic drugs and phototherapy also remain treatment options, including cyclosporine, methotrexate, azathioprine, and systemic corticosteroids (which are generally recommended against by most guidelines).9,11,12
In the UK, EU, and USA, there are four biological therapies currently approved for the treatment of moderate-to-severe AD: dupilumab, tralokinumab, lebrikizumab, and nemolizumab, and two small-molecule JAK inhibitors: upadacitinib and abrocitinib. JAK inhibitor baricitinib is also approved in the UK for the treatment of moderate-to-severe AD (Figure 2).7,9,10,13
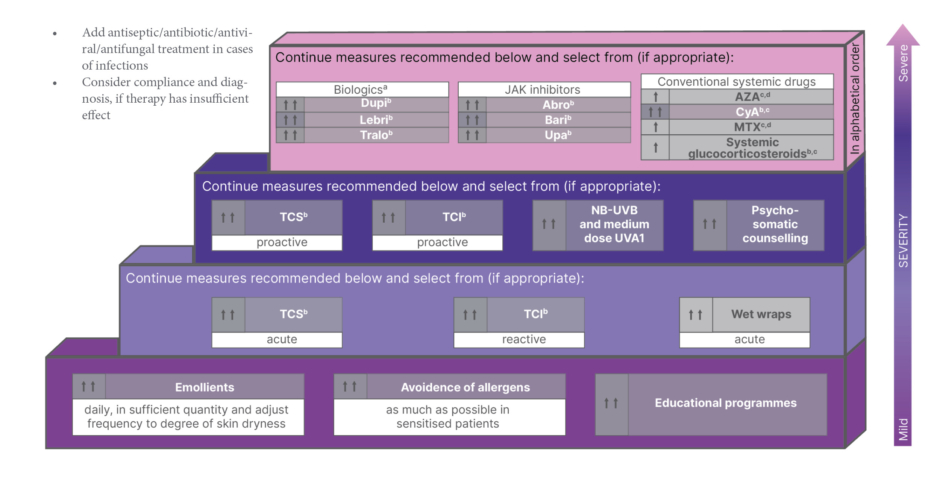
Figure 2: The EuroGuiDerm guideline on atopic eczema: stepped care plan.13
aNemolizumab has been approved in the EU for the treatment of atopic eczema since publication of Wollenberg, 2025.
bLicensed indication.
cRefer to guideline text for restrictions.
dOff-label treatment.
↑ Weak recommendation for the use of an intervention.
↑↑ Strong recommendation for the use of an intervention.
For definitions of disease severity, acute, reactive, proactive, see section VII and ‘Introduction to systemic treatment’ of the EuroGuiDerm Atopic Eczema Guideline.13
Adapted from Wollenberg et al.13
Abro: abroticinib; AZA: azathriopine; Bari: bariticinib; CyA: cyclosporin; Dupi: dupilumab; Lebri: lebrikizumab; MTX: methotrexate; TCI: topical calcineurin inhibitors; TCS: topical corticosteroids; Tralo: tralokinumab; Upa: upadacitinib; NB-UVB: narrow-band UVB.
Recent European (EuroGuiDerm) guidelines have recommended that patient eligibility for systemic therapy is not determined solely by objective disease severity, but by considering the magnitude of impairment of daily life activities and patient-reported QoL.13
JAK Inhibitors
Experts emphasised the role of JAK inhibitors alongside biologics when managing AD in high-burden areas,10,12 often utilised in cases where a more rapid treatment response is a need or is desired by the patients, particularly in those with AD affecting visible areas. JAK inhibitors also provide an alternative systemic treatment option for those who may be non-responsive or unsuitable candidates for biologic or conventional therapies.10 Clinical studies, including head-to-head comparisons with dupilumab, suggest that JAK inhibitors provide faster improvement of the signs and symptoms of AD than biologic therapy.14
Generally, safety data have been tolerable in the long-term treatment of AD with JAK inhibitors and broadly comparable to background epidemiologic populations.10,14 However, experts highlighted that treatment with JAK inhibitors comes with potential risk of major adverse cardiovascular effects, venous thromboembolism, and infections, as reflected in class warnings following safety signals identified in long-term trials of JAK-inhibitor treatment in older studies of rheumatologic disease.13 This also implicates different hurdles, such as the need for screening and monitoring of risk. Whilst treatment guidelines position JAK inhibitors alongside biologic therapies as systemic treatment options for moderate-to-severe AD, and newer generations of JAK inhibitors have not been evaluated for these warnings,15 experts noted that these risks continue to be a concern amongst peers, concluding that prescribing decisions should be informed by individual patient demographics, comorbidities, and overall benefit–risk profile.
The experts also agreed that, in certain settings, JAK inhibitors may be used as intermittent or short-term therapy. In contrast, biologic therapies are often preferred for long-term disease management due to their favourable long-term safety profile.10 Consequently, treatment selection often requires balancing the need for rapid symptom relief with patient-specific factors, including patient-reported QoL and desired outcomes, the occupational impact and daily functioning, patient comorbidities, risk of adverse events, and adherence, alongside broader healthcare considerations, including long-term safety, access to advanced therapies, and cost.10,16
Conventional Systemic Agents Are Still Frequently Prescribed
Despite the growing number of available targeted therapies, experts highlighted that conventional systemic agents, such as methotrexate and cyclosporine, continue to play an important role in clinical practice.10,13 They stressed that clinicians are increasingly beginning to adopt more flexible and combined treatment strategies to achieve optimal disease control in patients with AD affecting high-burden areas, who may not be responsive to traditional management approaches.
They emphasised that clinical decisions regarding the initiation of systemic treatment or switching to a biologic or JAK inhibitor, and vice versa, are typically based on overall disease severity, impact on QoL, and individual response to first- and second-line treatments.
UNDERSTANDING BIOLOGIC TREATMENT IN HIGH-BURDEN AREAS
Experts discussed the existing literature and ongoing clinical trials evaluating biologic therapies for sensitive, high-burden areas. They outlined that both RCTs and real-world evidence have demonstrated the robust safety profiles and durable, long-term efficacy of biologic therapies in patients with moderate-to-severe AD,16-18 with sustained reductions in signs and symptoms of the disease, as well as disease burden and QoL measures.19-24
Existing studies in AD affecting high-burden, sensitive areas are non-comparative and not designed as head-to-head trials; therefore, direct comparisons between therapies and definitive conclusions about relative efficacy cannot be drawn.
Biologic Treatment of High-Burden Areas: Dupilumab
Dupilumab, the first-approved biologic for moderate-to-severe AD, has had the most extensive trials and reported real-world evidence.16-19,25 Dupilumab treatment for AD affecting high-burden areas of the hands and feet has been investigated in Phase III clinical trials such as LIBERTY-AD-HAFT, a randomised, double-blind, placebo controlled RCT (N=133).25 Patients were randomised to dupilumab monotherapy (n=67) or matched placebo (n=66). Clinician and patient-reported instruments specific to assessing hand and foot disease severity were utilised in the study, such as the Hand and Foot Investigator Global Assessment (HF-IGA). Experts highlighted that the use of site-specific outcomes tools can be an important differentiator when using clinical trial data to inform real-world treatment decisions for AD in high-burden areas. Treatment with dupilumab resulted in significant improvements compared to placebo from baseline to Week 16, with 40.3% versus 16.7% (p=0.003) of patients reaching HF-IGA 0/1 at Week 16.25
Treatment-emergent adverse events were reported by 65.7% of participants in the dupilumab group and 74.2% in the placebo group; the most frequent adverse events were conjunctivitis and herpes infections among those randomised to dupilumab. Conjunctivitis events were assessed as non-serious and mild-to-moderate.25
Post-hoc analyses of the randomised, double-blinded, placebo-controlled dupilumab Phase III LIBERTY-AD-CHRONOS trial evaluated treatment response across four anatomical regions (head and neck, trunk, upper extremities, lower extremities), as assessed by the Eczema Area and Severity Index (EASI). Patients receiving 300 mg every 2 weeks plus TCS or placebo plus TCS were included in the post-hoc analysis. Dupilumab was found to significantly improve the severity of individual AD signs, which was comparable across all four anatomic regions and maintained through Week 52.26
In addition, the safety, effectiveness, and drug survival of dupilumab have been investigated in those registered to the Danish Nationwide SCRATCH registry (n=347) over 104 weeks.5,19 Patients treated with dupilumab and registered to SCRATCH were observed for improvement in AD severity, as measured by EASI. EASI scores at baseline were 18.0 (10.6–25.2) and, at Week 104, 1.7 (0.8–3.8).19 Of all patients, 35% reported an adverse event, with conjunctivitis (25%) as the most commonly reported.19 Drug survival was high at 86% after 2 years, but, paradoxically, dupilumab was found less effective in the high-burden region of head and neck, with 76% of patients reporting head and neck involvement at baseline, and 68% continuing to report head and neck involvement at Week 104.19
Biologic Treatment of High-Burden Areas: Tralokinumab
The long-term efficacy of tralokinumab as a monotherapy and in concomitant use with TCS has been assessed in patients with head and neck AD through a post-hoc analysis of ECZTRA 1 and 2 Phase III, and the ongoing ECZTEND open-label extension trial.20 In these Phase III, placebo-controlled trials, tralokinumab with and without TCS has shown favourable efficacy and safety profiles sustained over 2 years.20 The analysis was designed to evaluate long-term tralokinumab on head and neck AD and associated improvements in QoL. For the analyses, both overall EASI and head and neck EASI were evaluated. At parent trial baseline, median head and neck EASI was 3.0 (interquartile range: 1.8–4.5) and almost 90% of patients (n=1,060/1,192) had a head and neck EASI of ≥1.20
At Week 152, the number of patients with head and neck EASI ≤1 was 87.2% (232/266), with a median head and neck EASI of 0.4 and tralokinumab demonstrating sustained improvements in head and neck in patients with severe AD and significant head and neck involvement. Moreover, sustained improvements in head and neck AD were associated with QoL improvements, measured using DLQI, with the strongest correlations reported for questions regarding skin discomfort and embarrassment due to skin.20 Experts noted that long-term clinical data that incorporate QoL measures are valued when making treatment decisions.
A 36-week real-world study also assessed the effectiveness of tralokinumab on different anatomical sites and clinical signs in patients with moderate-to-severe AD (n=129).21 EASI scores were analysed on the whole body, four sites (head/neck, trunk, upper limbs, and lower limbs), and four clinical signs (erythema, oedema/papulation, excoriation, and lichenification) at 4, 12, 24, and 36 weeks. Tralokinumab was reported to reduce EASI scores consistently across various anatomical sites and clinical signs. Magnitude of decreasing EASI was highest on lower limbs, and achievement of EASI 75 at Week 36 was similar across all anatomical sites.21 The rate of achieving EASI 100 gradually increased from Week 4 through to Week 36 for the whole body and each anatomical site. The magnitude of increase appeared higher on head and neck (41.3%) and lower limb regions (40.3%) compared to the upper limbs (32.9%), trunk (25.3%), and whole body (21.4%).21
Regarding clinical signs, decreasing EASI and achieving EASI 75 or 100 was highest for excoriation and were 71.1%, 69.4%, 68.4%, and 60.5% for erythema, excoriation, lichenification, and induration/oedema/papulation, respectively.21 Additionally, real-world studies have shown that tralokinumab treatment is effective for head and neck AD in patients who have not responded to previous treatment with systemic therapies.22,23
The 32-week AD-HAND trial was a randomised, double-blind, placebo-controlled Phase IIIb trial investigating the efficacy and safety of tralokinumab in patients with AD with moderate-to-severe hand involvement (n=235).24 Data from Week 16 was presented at the International Society of Atopic Dermatitis (ISAD) 2025. Endpoints included proportion of responders with Investigator’s Global Assessment for atopic hand eczema (IGA-AHE) 0/1, and proportion of responders achieving Hand Eczema Severity Index (HECSI)-75 and HECSI-90, as well as patient-reported symptoms of itch, pain, sleep disturbance, and QoL. At Week 16, a significantly greater proportion of patients treated with tralokinumab achieved the primary endpoint of IGA-AHE 0/1 (clear or almost clear skin on the hands) compared with placebo (40.0% versus 10.6%, respectively; 95% CI; p<0.001).24 Moreover, a significantly greater proportion of patients treated with tralokinumab achieved HECSI-75 or HECSI-90 at Week 16 compared to placebo (65.1% versus 33.8% and 41.7% versus 10.9%, respectively; 95% Cl; p<0.0001).24
In regard to patient-reported QoL, at Week 16, patients treated with tralokinumab versus placebo reported statistically significant improvements, as measured by the DLQI and Hand Eczema Impact Scale (HEIS), as well as statistically significant improvements in itch and pain, as measured by the Hand Eczema Symptom Diary (HESD), compared with placebo. Overall, favourable safety and tolerability were reported, with no new safety signals identified.24
Recent data were also presented at ISAD 2025 on the real-world, prospective, non-interventional, international, single-cohort TRACE study, which evaluated the effectiveness of tralokinumab for the treatment of AD with genital involvement (n=124). The study evaluated changes in disease severity (EASI, Investigator Global Assessment [IGA], Scoring Atopic Dermatitis [SCORAD]) as well as patient-reported measures (QoL, itch, sleep) for up to 12 months.27 With improvements seen as early as Month 3, 78% of patients with AD involving genital areas at baseline had no AD on the genitals by Month 12.27 Substantial improvements were also seen in overall disease severity and QoL measures.27 Experts explained that in their clinical experience, AD affecting the genital area is likely to go underreported due to patient reluctance and embarrassment to raise the topic with clinicians, combined with a lack of routine examination in this region in practice.
Treatment of High-Burden Areas: Lebrikizumab
Phase III trials of lebrikizumab treatment in patients with moderate-to-severe AD have demonstrated robust efficacy, as shown in the ADvocate 1, ADvocate 2, and ADhere clinical trials. Post-hoc analyses have been carried out to evaluate outcomes in patients specifically with facial and hand involvement.28,29
Results of exploratory post-hoc analyses ADvocate 1 and ADvocate 2 were presented at the British Association of Dermatologists (BAD) in 2023. Lebrikizumab 250 mg monotherapy was compared with placebo while ADhere assessed lebrikizumab in combination with TCS versus TCS alone over 16 weeks.28 Clinician-assessed change from baseline was categorised as cleared, improved, no change, or worsened, with significant improvements in facial and hand dermatitis observed with lebrikizumab at Week 16.
Additional post-hoc analyses of the ADvocate 1 and 2 studies evaluated treatment efficacy across anatomical regions using EASI scores for the head and neck, upper extremities, trunk, and lower extremities.29 Patients receiving lebrikizumab demonstrated significantly greater improvements compared with placebo across all body regions.29 Ongoing research will further evaluate the efficacy of lebrikizumab in AD affecting the hands and feet in the ADtouch study.30
UNMET NEEDS IN HIGH-BURDEN AD PERSIST
Clinical Scoring Methods
Commonly used AD severity scoring measures, such as the EASI and SCORAD, were highlighted by the experts as having limitations when it comes to assessing high-burden areas. As typical AD severity scoring systems tend to be size-weighted, smaller but high-burden, sensitive areas such as the head and neck, face, scalp, hands, and feet may be underrepresented in evaluations. As a result, the disease burden experienced by patients may be underestimated. Moreover, patients with disease localised to smaller but highly burdensome regions may also be underrepresented in clinical trials that investigate systemic therapies in moderate-to-severe AD. This is largely due to eligibility criteria that prioritise overall disease severity, such as minimum body surface area involvement (often ≥10%) and EASI threshold, which experts agreed may exclude patients whose disease may be affecting a smaller surface area but still has a high burden.
In recent studies investigating biologic and JAK inhibitor treatment for AD, the site-specific score HECSI has been utilised.19,24,25,31 Experts agreed on the usefulness of clinical trials that utilise site-specific scores to measure treatment efficacy in high-burden areas, which help to inform real-world treatment decisions, but also highlighted that these site-specific score approaches are not yet routinely implemented or standardised across clinical trials or within clinical practice.
The experts agreed that existing site-specific scoring tools, such as HECSI, are complex and granular, which, despite their usefulness in clinical trials, may limit their practical application in the real-world and perceived usefulness from a patient perspective. As a result, currently available outcome measures do not fully reflect the heterogeneity of AD, especially the specific burden associated with disease in high-impact locations. In addition to site-specific scoring tools, experts agreed that multidimensional treat-to-target approaches are useful, assessing a combination of patient-reported and clinician-reported outcomes and incorporating QoL measures.31-33
Overall, experts agreed that in clinics and real-world evidence, it is clear that moderate-to-severe AD in visible, sensitive, difficult-to-treat, and overall high-burden areas has a significant effect on patients’ lives.3,4,6 They concluded that clearer definitions and an improved understanding and awareness amongst clinicians is crucial to ensure that AD in high-burden areas is appropriately recognised and assessed.
The Need for Directed Research in High-Burden Areas of AD
Despite the recognised substantial disease burden experienced by patients with high-burden area involvement, experts emphasised the lack of directed research on high-burden areas, with limited trials and tools evaluating treatment efficacy specifically focused on the head and neck, face, scalp, feet, hands, and genitals. Despite important contributions of ongoing Phase III trials specifically focused on AD impacting the hands, and incorporation of site-specific measures such as HECSI, experts agreed that comparative trial data to evaluate and compare the efficacy of biologics in high-burden, sensitive anatomical areas would be pivotal in informing treatment decisions.
Overall, experts emphasised the need for further dedicated, prospective, and long-term clinical trials specifically designed to investigate the treatment of AD in high-burden areas. The experts shared that, currently, much of the evidence used to inform clinical decision-making in these high-burden areas is derived from post-hoc analyses or shared clinical experience within specialist practice, highlighting a clear gap for further research. In addition, there are no head-to-head comparator studies between biologics, so clinical decision-making for patients with high-burden AD often relies on existing data combined with anecdotal clinical experience.
Overarching Treatment Access Barriers
A common, more encompassing issue highlighted by the experts in the roundtable discussion was access to treatment. In real-world clinical practice, experts noted that the choice of therapy for high-burden AD is largely shaped by availability in any given country or healthcare system. In 2021, a USA patient survey was carried out to assess unmet needs in patients with moderate-to-severe AD, conducted online. Of those with self-reported moderate-to-severe AD (n=1,935), 51% (n=979) reported inadequate control of their AD. Of those reporting inadequate control, an enriched survey revealed that over half had never received dupilumab (n=178/284).34 This reflected the experts’ shared view that biologics are likely underused in eligible patients with moderate-to-severe AD.
Access to advanced therapies remains uneven across healthcare systems. In some settings where access to biologics is limited, JAK inhibitors may be used intermittently. Experts also highlighted a degree of therapeutic inertia amongst clinicians, particularly those in general practice rather than specialist clinics, who may remain hesitant to initiate systemic therapies for patients with moderate-to-severe AD. It was also highlighted that outside of specialist clinics, clinicians may not routinely assess for high-burden area involvement, which can contribute to under-recognition and suboptimal management, emphasising the importance of education for clinicians, as well as education for patients.
As a result, experts emphasised that not only improving access to therapies, but delivering education to clinicians about recognising the impact of AD in high-burden areas and utilising available options remains a key unmet need to overcome in the real-world management of AD.
The Importance of Patient Education, Support, and Communication
As an overarching theme throughout the roundtable discussion, experts emphasised that patient communication and shared decision-making should form central pillars when managing AD, particularly in patients with AD affecting high-burden, sensitive anatomical sites. As mentioned prior, traditional scoring tools may not fully capture the severity of psychosocial burden, and, as a result, experts agreed on the importance of actively listening to patients and understanding which symptoms and treatment outcomes matter to them.35,36
From the roundtable discussions, it was clear that patients often prioritise skin clearance, symptom relief, long-term control, and safety, reflecting the desire for stable disease management rather than reactive, ad hoc treatment of flares. The experts noted that, by achieving an understanding of the patient’s desired treatment goals, the patient is more likely to adhere to their medication. Incorporating patient-reported outcomes, including measures of QoL, itch, sleep disturbance, and fatigue (e.g., Functional Assessment of Chronic Illness Therapy [FACIT]), as well as consideration of anxiety, depression, and patient satisfaction, was also agreed to be important for guiding treatment escalation and/or switching, enabling clinicians to adjust treatment based on disease severity.
In addition to establishing patient and clinician education on treatment options, the need for greater psychological and psychosocial support for patients remains crucial to the holistic management of AD in high-burden areas.37,38 Overall, experts stressed that initiating treatment is key, but that does not mean the battle is won. Successful long-term disease management requires a comprehensive, patient-centred approach.
FUTURE OUTLOOKS FOR AD IN HIGH-BURDEN AREAS
Individualised Therapy
Looking to the future, the experts expressed hope for the evolving disease landscape and the future of individualising therapy for patients. As treatment strategies begin to move towards an era of precision medicine, experts emphasised that a detailed understanding of immunological pathophysiology underlying different AD subtypes, particularly those that are high burden, may aid clinicians in the selection of treatment for patients who may respond better to certain therapies, exhibit better durability, or may be more prone to relapsing.
As an example, IL-22 and thymus and activation-regulated chemokine (CCL17/TARC) are biomarkers for which early research has shown correlates with disease severity.39,40 Evidence points to strong upregulation of IL-22 in the skin of patients with AD, which is associated with the proliferation of keratinocytes and dysfunction within the epidermal barrier, raising the potential of blockading IL-22 as a therapeutic target.39 Moreover, existing biologic therapies have been observed to reduce serum levels of TARC before visible clinical improvements,40,41 indicating the potential of the serum biomarker as an early indicator of therapeutic efficacy. More research is needed to clearly define these biomarkers.
The incorporation of specific AD phenotypes into clinical trials may therefore provide valuable guidance for clinicians when selecting and monitoring outcomes for the most appropriate therapy for patients with moderate-to-severe AD in high-burden areas. Additionally, recent research into emerging genetic expression profiling options may be able to guide therapeutic decisions based on profile analysis.42
CONCLUSION
To conclude the roundtable discussion, experts agreed that the ultimate goal in AD, and AD affecting high-burden areas, remains true sustained disease control, remission with minimal disease burden, and favourable long-term safety. Despite advances in systemic and biologic therapies, significant unmet needs persist among patients with high-burden, difficult-to-treat, sensitive areas, where maintained disease control and successful long-term management of both clinical signs and QoL remain challenging.
In conclusion, experts emphasised the importance of personalised treatment strategies for each patient, looking ahead to the future use of biomarkers to better understand treatment response and guide therapy selection. The availability of robust, comparative, directed clinical data of systemic therapies on AD in high-burden areas would further support optimal treatment selection. Addressing these limitations, alongside continued patient and clinician education and shared decision-making, will be critical to ensuring the effective management of AD in high-burden areas.






